
WASHplus in Mali: integrating WASH and nutrition for healthy communities
By Renuka Bery, Sahada Traore and Lonna Shafritz
Renuka Bery is the Integration Manager of the WASHplus project managed by FHI 360. She currently oversees the WASHplus WASH-nutrition programme in Mali and a WASH and Neglected Tropical Diseases programme in Burkina Faso.
Sahada Traore, a WASH specialist, works for CARE Mali and is the Mali Project Director for the WASH and nutrition programme. He has authored and co-authored several short films and texts around WASH.
Lonna Shafritz, Senior Technical Advisor with FHI360, currently manages the WASHplus Mali programme. She has extensive worldwide experience providing technical guidance on behaviour change, training and evaluation activities in WASH, nutrition and other topics, including environment and wildlife.
WASHplus would like to thank USAID, in particular USAID/Mali, for its support of this programme.
Location: Mali
What we know: Undernutrition remains prevalent in Mali; food insecurity and inadequate water, hygiene and sanitation are two important contributing factors.
What this article adds: In 2012, an integrated water, sanitation, and hygiene (WASH) and nutrition project was initiated by CARE (part of USAID WASHplus project) in northern Mali. It revolves around community-led total sanitation (CLTS) using behaviour-change approaches to improve nutrition and hygiene practices. Activities include hygiene promotion, water treatment, breastfeeding counselling, media and advocacy, and identification/referral of malnourished cases. Achievements include improved regional policies; increased district capacity on WASH and nutrition interventions; and improved community infrastructure and practices around women and child health. Local stakeholders have proved critical to success. Endline results are due in 2016.
Background
 Mali is currently ranked 179 out of 188 countries on the 2015 Human Development Index. It has one of the highest fertility rates in the world at 6.6 children per woman (USAID, 2014) and a 2015 child mortality rate of 115 per 1,000 live births (World Bank). The country experiences food insecurity and hunger. Poverty and food insecurity that contribute to undernutrition rates – wasting prevalence is 15% (State of the World’s Children, 2015) – have changed little in Mali and are exacerbated by inadequate feeding practices; most children are not exclusively breastfed, and few children under two receive a minimum acceptable diet (USAID, 2014).
Mali is currently ranked 179 out of 188 countries on the 2015 Human Development Index. It has one of the highest fertility rates in the world at 6.6 children per woman (USAID, 2014) and a 2015 child mortality rate of 115 per 1,000 live births (World Bank). The country experiences food insecurity and hunger. Poverty and food insecurity that contribute to undernutrition rates – wasting prevalence is 15% (State of the World’s Children, 2015) – have changed little in Mali and are exacerbated by inadequate feeding practices; most children are not exclusively breastfed, and few children under two receive a minimum acceptable diet (USAID, 2014).
The causes of undernutrition are complex, varied and many, including inadequate WASH and nutrition-related behaviours. The behaviours result from a range of factors: insufficient information on appropriate hygiene and nutrition practices, along with poverty, lack of key critical supplies and services and food insecurity. Cultural practices and social norms, such as extended family dynamics and unequal gender relations, also affect family food allocation.
Project overview
The WASHplus project, led by FHI 360 with CARE/USA as a core partner, creates and supports interventions that lead to improvements in WASH and explores and promotes innovation in the WASH sector, including integrating WASH into related sectors such as nutrition (see Box 1). In 2012, USAID/Mali requested that the WASHplus project submit a plan for an integrated WASH and nutrition project in the Mopti region. WASHplus subsequently targeted 180 villages in 18 communes in three districts (Mopti, Bandiagara and Bankass) in northern Mali, USAID’s priority areas. The programme benefits from CARE’s presence in each district; however, the communes selected had not yet received WASH programming.
Box 1: About WASHplus
The WASHplus project supports households and communities by creating and delivering interventions that lead to significant improvements in access, practices, and health outcomes related to WASH and household air pollution (HAP). This multi-year project (2010-2016), led by FHI 360 in partnership with CARE and Winrock International, is funded through USAID’s Bureau for Global Health. WASHplus has been engaged in Bangladesh, Benin, Burkina Faso, Kenya, Liberia, Madagascar, Malawi, Mali, Nepal, Uganda and Zambia.
The objectives of the WASHplus project are to:
- Reduce diarrhoeal diseases and acute respiratory infections in countries, using at-scale approaches;
- Integrate WASH and HAP interventions into education, HIV/AIDS, maternal and child health, and nutrition programmes;
- Promote innovation; and
- Foster strong in-country partnerships.
WASH and HAP are integrated with other health and non-health programmes to expand uptake and sustainability of WASH and HAP services. The project tests behavioural, programmatic and technological innovations and fosters creative partnerships to enhance funding, advocacy and impact for WASH and HAP improvement.
For more information, visit: www.washplus.org
Working through CARE Mali, the overall goal of WASHplus in Mali is to improve the nutritional status of 187,000 women of reproductive age and 60,000 of their children (especially those under two) in poor, rural households and communities. The programme had three objectives to reach this goal:
- Increase supply of appropriate, affordable, and sustainable WASH solutions;
- Increase demand for low-cost sanitation; and
- Improve sanitation and hygiene practices and nutrition behaviours.
 Implementation villages were selected using a participatory methodology orchestrated by the government to allow for transparency using an objective, needs-based approach that avoids duplication with other development partners working in the same communes. The process also effectively garnered broad institutional support among government stakeholders in the district offices of health, water, and sanitation.
Implementation villages were selected using a participatory methodology orchestrated by the government to allow for transparency using an objective, needs-based approach that avoids duplication with other development partners working in the same communes. The process also effectively garnered broad institutional support among government stakeholders in the district offices of health, water, and sanitation.
Stunting, wasting, mid-upper arm circumference (MUAC) and diarrhoea prevalence will be measured at endline, along with WASH and nutrition practices and WASH supplies (anthropometry was not measured at baseline). Results will be available March/April 2016.
Project activities
WASHplus’s core activity revolves around Community-Led Total Sanitation (CLTS). The project emphasises improving nutrition and hygiene practices through a range of behaviour-change approaches. It also identifies undernourished children who are referred to the community health/nutrition centres for treatment.
CLTS+
CLTS+ is a participatory approach to improve access to and use of latrines and eliminate open defecation. Community members analyse their traditional sanitation practices and discuss publicly what happens to all that ‘shit’ in the environment. Effective CLTS community ‘triggering’ events ‘ignite’ a sense of shared disgust and shame when members realise they are ingesting one another’s faeces. This spurs latrine construction at the village level. WASHplus introduced a CLTS+ approach that also promoted hand-washing with soap.
Since CLTS is a process rather than a one-time community mobilisation event, WASHplus established a calendar for monitoring visits. Village sanitation committees and facilitators monitor villages that have not yet reached open defecation-free (ODF) status even after being triggered. The external monitoring by commune, district and regional staff helps to maintain community commitment to latrine construction and serves to reinforce important hygiene messages such as washing hands with soap, exclusive breastfeeding until six months, and complementary feeding for children over months.
 Latrine construction in rural communities has proved challenging because different geographic areas required different types of latrines, depending on the soil type. In areas that have a high water table or are flood-prone, the pits are shallow and fill quickly. In sandy soils, the pits tend to collapse during the rainy season, and in the rocky soil of the Dogon Plateau the population could not dig holes by hand. Thus, WASHplus and technicians from the public health offices in each district designed new latrine models to fit the geological context. Two masons from each village were trained in latrine construction. The masons learned simple techniques to identify the type of pit required, protect the wood, and strengthen the waterproofing of the slab. Training masons before triggering the villages ensured that when households were ready masons were able to construct the latrine for a small fee using materials secured by the villager.
Latrine construction in rural communities has proved challenging because different geographic areas required different types of latrines, depending on the soil type. In areas that have a high water table or are flood-prone, the pits are shallow and fill quickly. In sandy soils, the pits tend to collapse during the rainy season, and in the rocky soil of the Dogon Plateau the population could not dig holes by hand. Thus, WASHplus and technicians from the public health offices in each district designed new latrine models to fit the geological context. Two masons from each village were trained in latrine construction. The masons learned simple techniques to identify the type of pit required, protect the wood, and strengthen the waterproofing of the slab. Training masons before triggering the villages ensured that when households were ready masons were able to construct the latrine for a small fee using materials secured by the villager.
Rehabilitation of water access points was planned to incentivise villages to become ODF. At the start of the project, WASHplus inventoried the existing water points in the target villages and identified problems. Villages were ranked by district and by commune based on their CLTS+ progress. In each district, the first two villages in each commune to reach ODF status were selected to have their water point rehabilitated or to receive a new water point. This competition helped motivate communities to become ODF quickly. WASHplus intends to assist all villages that have reached ODF status to rehabilitate at least one water point by the end of the project.
Behaviour change efforts/hygiene promotion
Community health workers, called relais, play an important role in the Malian health system as messengers of information and promoters of healthy behaviours. WASHplus works closely with relais to promote behaviour change at the household and community levels and to offer support, outreach and extension services to the commune health clinics. WASHplus organised training and capacity-building sessions and taught relais how to negotiate improved behaviours with mothers, using Ministry of Health-approved WASH-nutrition job aids that WASHplus developed to facilitate behaviour change. A competition was initiated among target villages to create and use tippy taps to promote hand-washing.
The relais use the existing women’s groups – village savings and loan associations (VSLA) – as entry points to promote improved nutrition and hygiene behaviours. During household visits, relais counsel caregivers on practices such as hand-washing with soap; safe treatment and storage of drinking water; exclusive breastfeeding; complementary feeding; and safely disposing of faeces. Relais organise awareness-raising sessions with community groups using the WASH-nutrition job aids. After the Ebola virus was detected in Mali, WASHplus integrated Ebola messaging into the training.
Water treatment
 WASHplus, in collaboration with the Regional Directorate of Health, trained community health workers in different point-of-use water treatment methods. They further refined the materials and cascaded the training to all community health workers and community health agents in the 18 project communes. In 2015, WASHplus began conducting water treatment demonstrations using PUR which clearly showed that unprotected water in villages is not safe. (PUR is a water purification technology developed by Proctor and Gamble and applied in collaboration with the U.S. Centers for Disease Control and Prevention. The water purification packet contains a powdered mixture that removes pathogenic microorganisms and suspended matter, making previously contaminated water clean.)
WASHplus, in collaboration with the Regional Directorate of Health, trained community health workers in different point-of-use water treatment methods. They further refined the materials and cascaded the training to all community health workers and community health agents in the 18 project communes. In 2015, WASHplus began conducting water treatment demonstrations using PUR which clearly showed that unprotected water in villages is not safe. (PUR is a water purification technology developed by Proctor and Gamble and applied in collaboration with the U.S. Centers for Disease Control and Prevention. The water purification packet contains a powdered mixture that removes pathogenic microorganisms and suspended matter, making previously contaminated water clean.)
Exclusive breastfeeding
The project promotes exclusive breastfeeding in two steps. First, the relais visit VSLA and use the counselling cards to talk with new mothers about the importance of exclusive breastfeeding. Second, the relais identify champions during these visits and use these women to conduct household visits to support breastfeeding mothers and promote exclusive breastfeeding to other family members, such as husbands and mothers-in-law. Radio spots and live debates support these messages.
Nutrition demonstrations
Nutrition demonstrations show parents the possibilities of expanding children’s diets by introducing locally available and affordable food products. WASHplus trained community health workers and agents to organise and lead nutrition demonstrations at the commune and village levels, as well as at community health facilities. The demonstrations discuss infant and young child feeding practices, including how much children of different ages should be eating. In addition, they classify foods and food groups so parents understand the importance of feeding children a variety of foods. The majority of the demonstrations promote enriched porridge made of millet, beans, peanuts, salt, sugar, baobab tree fruit, or tamarind – a nutritious meal that can be made with affordable, readily available foods. WASH is integrated into these demonstrations; hand-washing with soap before touching food is modelled and point-of-use water treatment is demonstrated or discussed.
Media and advocacy
WASHplus developed a radio strategy to improve communication and raise awareness about WASH and nutrition. Each radio station uses a weekly time slot to broadcast the results of CLTS+ monitoring visits in local languages to create a sense of friendly competition among the villages. The station then hosts debates with local champions. Radio spots also advise taking severely malnourished children to health centres. These programmes are helping to maintain community momentum around constructing and using latrines and screening for malnourished children.
WASHplus has worked closely with the regional directorates for health, sanitation and water services to plan celebrations of the various global days related to WASH and nutrition. In addition, WASHplus showcased its activities and innovations at a national forum on water and sanitation, as well as at regional WASH dialogues that fed into a national event.
Nutrition referrals and support for accompanying caretakers
During their household visits, relais screen children under five for malnutrition by measuring MUAC. Severely and moderately malnourished children are triaged and referred to health centres. Health centre personnel also attend village events and screen children. WASHplus supports health workers at the referral centres to screen children and enter data into registers. When WASHplus began to refer children in January 2013, 17% in Bankass and 6% in Bandiagara did not attend the health centre because caretakers could not afford to go. To promote adherence, WASHplus began to cover the transport and food costs for caretakers of all children with complications; now families bring their children to the referral centres. Children without complications are treated directly in the villages or at the community health centres, so travel is not an issue.
Project accomplishments
After 30 months of implementation, WASHplus has progressed toward accomplishing its objectives: improved policies adopted at the regional level that may become national standards; increased capacity within the intervention districts to provide WASH and nutrition interventions; and improved infrastructure and practices at the community level that will help to enhance the health outcomes of women and children in the targeted villages.
Policy
The Mali Government’s national CLTS policy was updated to incorporate the WASHplus-developed latrine options for different zones: flood-prone, sandy and rocky. Further, the Government has advocated that masons be trained prior to CLTS triggering to ensure that demand for latrine construction is met in a timely and responsive manner. WASHplus is also working with the Government to improve the training guide for post-ODF action planning; first to develop a module to help CLTS facilitators revitalise WASH committees and implement a sustainability plan; and second to promote tree planting to mitigate the effects of constructing traditional latrines using wood.
Increased capacity
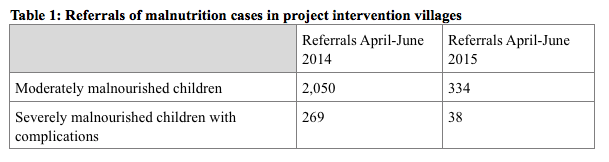
WASHplus has trained over 400 community extension workers to negotiate improved WASH and nutrition practices at the household level in 180 villages. Activities include CLTS triggering and nutrition and water treatment demonstrations at the community level and individual household visits that focus on promoting exclusive breastfeeding, hand-washing with soap, and nutrition counselling and referrals. These workers regularly monitor and refer malnourished children in project intervention villages. In the target areas the number of children referred has diminished drastically as shown in Table 1. The reduction in referrals is attributed to the early detection of growth faltering in communities through regular village screenings and treatment given at the community health centre before severe malnutrition occurs. It also could indicate that the health of children has improved while food insecurity has decreased. The endline survey may help to clarify the reasons behind this dramatic fall in referrals.
Improved community infrastructure and practices
Communities have eagerly embraced the ODF village concept. To date, over 75% of villages triggered by WASHplus have been certified as ODF. Within these communities, almost 10,000 latrines have been constructed, rehabilitated or upgraded since the start of this project and over 2,000 existing latrines without a hand-washing device have been equipped with one. Several villages also built communal latrines in farms, gardens, schools and markets to ensure the community remains ODF. Almost 50 water points have been constructed or rehabilitated to ensure communities have access to water. Furthermore, households now understand that most water is not safe to drink and are purchasing water treatment tablets (over 30,000 tablets per quarter). With project support, communities are planting fruit trees to mitigate the environmental impact of using wood to build latrines. To date, 8,300 fruit trees, which can further improve nutritional status, have been planted.
To sustain ODF status, WASHplus assisted the first 100 ODF communities to develop post-ODF action plans. All the communities have implemented these plans. WASHplus has also assisted all ODF villages to improve their environmental sanitation.
Lessons learned
Local stakeholders are critical to success
 WASHplus Mali engaged local stakeholders at different levels throughout the process of implementing the WASH-nutrition interventions. Community leaders and local government officials were all involved in making decisions and monitoring implementation and thus had a stake in seeing progress and success. Facilitating community discussions using the participatory decision-making approach helped to develop sustainable local systems to finance operation and maintenance costs of water points and triggered income-generating activities that also improve health behaviours. Involving masons from the community in producing new designs of cheaper, traditional latrines adapted to the environment was embraced by communities. Monitoring visits revealed that masons trained to construct low-cost latrines continued to innovate to adapt their products to the local context. These masons are being viewed as change agents in the villages. They take great pride in their work and are dedicated to achieving universal latrine coverage in the villages they serve.
WASHplus Mali engaged local stakeholders at different levels throughout the process of implementing the WASH-nutrition interventions. Community leaders and local government officials were all involved in making decisions and monitoring implementation and thus had a stake in seeing progress and success. Facilitating community discussions using the participatory decision-making approach helped to develop sustainable local systems to finance operation and maintenance costs of water points and triggered income-generating activities that also improve health behaviours. Involving masons from the community in producing new designs of cheaper, traditional latrines adapted to the environment was embraced by communities. Monitoring visits revealed that masons trained to construct low-cost latrines continued to innovate to adapt their products to the local context. These masons are being viewed as change agents in the villages. They take great pride in their work and are dedicated to achieving universal latrine coverage in the villages they serve.
Demonstrations expose problems and help define solutions
The project found that demonstrating water treatment with PUR powder visibly showed that water is not safe, which reinforced the need to treat drinking water. Showing men and women in the community how to prepare nutritious recipes using local products encourage families to accept and adopt such improved practices. Engaging community champions to convey new ideas in radio programmes increased understanding and encouraged healthy competition between communities in implementing good WASH practices.
Competition spurs action and innovation
WASHplus found that inciting competition among communities was effective in changing behaviour and achieving results in a short timeframe. It also helps maintain a community’s momentum. Further, providing incentives to benefit the community, such as rehabilitating a broken water point, encouraged them to move quickly. One community used village funds to purchase chlorine products and then established a sanitation shop in the village to provide regular access to these products. Another village created a sanitation store to provide durable latrine covers. Households that did not purchase a cover or used a damaged cover were fined. Finally, the villagers of Yarou Plateau emulated its neighbours from nearby Gouna by building latrines, sweeping the whole village every Thursday, and treating drinking water that resulted in reduced incidences of diarrhoea and a clean community.
WASH-nutrition integration presents challenges but offers promise
Anecdotal evidence from this project indicates that the integrated programming has positively influenced behaviours and health. Village women see changes in their children’s health; households are purchasing water treatment to ensure drinking water is not contaminated; communities are building latrines in fields and at bus stations to prevent open defecation; and other communities are cleaning their villages of plastic and animal waste and becoming entrepreneurs by creating businesses to support nutrition and hygiene.
Conclusions
Attributing reduced undernutrition to WASH-focused activities in general is difficult. Even if WASH programmes collect anthropometric indicators such as stunting or wasting, which most do not, it is difficult to determine to what extent the inclusion of WASH interventions has influenced changes in nutritional status and growth. Measuring such changes requires much more sophisticated evaluation design and analysis. In addition, detecting changes in stunting, for example, often requires timeframes longer than typical WASH programmes and funding cycles (this programme was initially planned for a two year period, hence baseline anthropometry was not included). While evidence exists to support WASH and nutrition integration, more data are needed to demonstrate how and in which ways specific WASH mechanisms affect nutrition outcomes and determine which implementation modalities are most likely to lead to strong and sustained impact. WASHplus will collect endline data that will help answer some of these questions, but because the project did not collect anthropometric data at baseline, it can only compare the differences in stunting and wasting between intervention and control communities at the endline.
The WASHplus project in Mali ends in April 2016. Efforts are underway to document the lessons learned and harmonise the WASH-nutrition materials so that partners who continue to provide WASH and nutrition services can build their programmes on things that have worked or not. WASHplus is actively sharing experiences with the government and USAID implementing partners, including exchange visits and preparing written and visual materials, as well as sharing experiences globally to the extent possible.
For more information, contact: Renuka Bery or tel: +1.202.884.8985
References
State of the World's Children (2015).
USAID: Mali Nutrition Profile (2014).
World Bank, Under 5 Mortality Rate.