
Assessment of adolescent girl nutrition, dietary practices and roles in Zimbabwe
.jpg?w=225 "IMC, 2015") Amelia Reese-Masterson and Pamela Murakwani
Amelia Reese-Masterson and Pamela Murakwani
Amelia Reese-Masterson has been with International Medical Corps since November 2011 as Research Advisor in the Nutrition, Food Security and Livelihoods Unit. She has over six years’ experience working in applied maternal and child health and nutrition research and programming. She holds an M.P.H. from Yale School of Public Health, with a focus in nutritional epidemiology.
Pamela Murakwani is the Country Director for International Medical Corps in Zimbabwe and Lead Nutrition Specialist for the USAID-funded Amalima Development Food Assistance Programme in Zimbabwe. She has over five years’ experience working in integrated nutrition programmes. She holds a Master’s degree in Public Health Nutrition from the London School of Hygiene and Tropical Medicine, United Kingdom and a BSc in Nutrition from the University of Zimbabwe.
This assessment was made possible through internal International Medical Corps funding and was further facilitated through the Amalima programme in Zimbabwe and technical support from staff at headquarters and in Zimbabwe. We acknowledge the study coordinator, Zothile Mlobane, and the team of survey data collectors and enumerators. We also acknowledge the Ministry of Health and Child Care (MoHCC), Zimbabwe and the Local Government and Rural District Council offices for approving this assessment and recognising the importance of increased knowledge of adolescent girl nutrition and health in Zimbabwe. Finally, we acknowledge the technical support received from Terri Ballard and Mark Nord at the Food and Agriculture Organization (FAO), Bradley Woodruff (Columbia University) and Kristen Cashin (FANTA).
Location: Zimbabwe
What we know: Adolescence is a period of heightened nutritional need, which can be compounded by pregnancy. There is a gap in knowledge to help guide programming priorities for adolescent nutrition, including in programme areas where International Medical Corps operates in Zimbabwe. Research has shown that menarche (or puberty) may be an opportunity for catch-up growth.
What this article adds: A recent study (cross-sectional survey and focus group discussions) examined adolescent girl nutrition, dietary practices and roles in four districts of Zimbabwe. Pregnancy was common (27%) and mostly outside marriage (89%) amongst 692 adolescent girls surveyed (13-19 years of age). Average age at first marriage was 16.6 years. Only 36% of the sample was attending school. The overall women’s dietary diversity score was 3.2. Nearly half (47%) of those surveyed were food-insecure and 66% had poor dietary diversity, which significantly correlated. However, rates of stunting and thinness were under 10%. Correlation between menarche and stunting (17.7% pre-menarche, 2.3% post-menarche) was significant (p<.001), although the sample size was small. Key influencers were aunts (pregnancy and contraception), mothers (food preparation and purchase, health-seeking) and parents (schooling). Nutrition and hygiene knowledge was low. Recommendations include integrated behaviour change at key contact points, interventions to retain girls in schooling, and adolescent-sensitive food security programming to address dietary diversity. Much further research is needed, including how to engage men and adolescent boys in avoiding early pregnancy, mid-upper arm circumference (MUAC) cut-offs, and adolescent reference populations for nutritional status assessment.
Adolescence is a period of heightened nutritional need, which can be compounded by pregnancy with its additional demands on a mother’s nutrient stores. The Lancet 2013 series on maternal and child nutrition identifies adolescent girls as a priority focus area for research and programming, due to the dearth of evidence available to inform adolescent nutrition interventions and the importance of ensuring nutritional wellbeing in this age group through puberty and going into motherhood. In recognition of this global need, and in response to the Zimbabwe Ministry of Health and Child Care (MOHCC)’s noted gap in knowledge to help guide programming priorities for adolescent nutrition, International Medical Corps carried out a study in June 2015 to examine adolescent girl nutrition, dietary practices and roles in Zimbabwe. The objectives of this assessment were to: 1) Describe nutrition-related beliefs, knowledge and practices among adolescent girls; 2) Assess adolescent girl nutrition, food security and dietary diversity status; 3) Identify potential risk factors related to poor adolescent nutritional status; and 4) Identify and characterise ‘key influencers’ who contribute to determining adolescent girl roles and responsibilities around nutrition.
Programme background
International Medical Corps is the technical lead for nutrition and health components of the USAID-funded Amalima programme (2013-2018), a five-year Development Food Assistance programme being implemented by Cultivating New Frontiers in Agriculture (CNFA), International Medical Corps, The Manoff Group, Organisation of Rural Associations for Progress (ORAP), Africare and Dabane Trust in two provinces in Zimbabwe; Matabeleland North and Matabeleland South. The programme is being implemented across four districts (Tsholotsho in Matabeleland North and Bulilima, Mangwe and Gwanda in Matabeleland South), with a goal to improve household food and nutrition security. Strategic objectives include: 1) Improved household access to and availability of food; 2) Improved community resilience to shocks; and 3) Improved nutrition and health among pregnant and lactating women and boys and girls under two years of age.
While there are currently no Amalima activities specifically designed to address the nutritional needs of adolescent girls (beyond the wider programme activities, in which adolescent girls may participate), International Medical Corps staff have noted significant numbers of pregnant teenage girls and young mothers, with programme staff noting anecdotally girls as young as 14 years. This indicates early sexual debut, possibility of school drop-out and increased risk of maternal morbidity and mortality. International Medical Corps recognises the need for tailored services for adolescent girls through a life-cycle approach that would ensure good nutritional practices and status throughout the adolescent period and better prepare them going into the critical ‘1,000 day window of opportunity’ from conception to second birthday.
Study methods
The assessment utilised both quantitative and qualitative data-collection methods. A cross-sectional survey was carried out among adolescent girls aged 13-19 years (n=692), using multi-stage cluster sampling, representative of selected wards in Mangwe and Tsholotsho districts. The questionnaire included demographics, dietary beliefs and practices, sexual and reproductive health, health access, food security, dietary diversity, WASH (water, sanitation and hygiene), community involvement and anthropometric measurements. Data were analysed in SPSS (Statistical Package for the Social Sciences) looking at descriptive statistics, correlations and difference in means. Further analysis of the Food Insecurity Experience Scale (FIES) data was conducted by the Food and Agriculture Organization (FAO) to look at the quality and comparability of the measure (Reese-Masterson et al, 2015). Qualitative data were collected by trained facilitators through focus group discussions (FGDs) and key informant interviews (KIIs) with adolescent boys (two FGDs, two KIIs), mothers/mothers-in-law (three FGDs) and fathers (two FGDs) of adolescent girls, as well as with adolescent girls (one FGD, one KII). There was an average of 10 participants across all groups. Qualitative data were analysed for themes and subthemes through an iterative process.
Findings
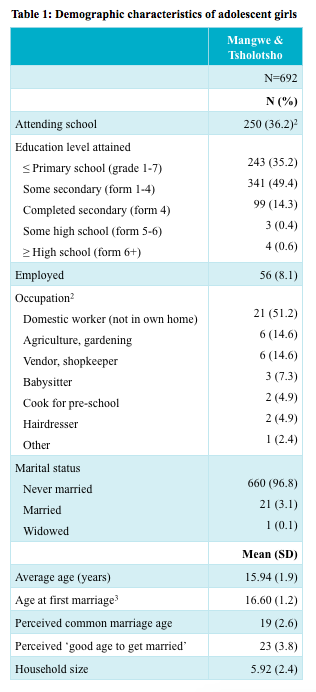
For the survey assessment, 692 adolescent girls aged 13-19 years (average age 15.94, SD 1.9) were interviewed in Tsholotsho and Mangwe districts, with a response rate of 98.5% (10 total refusals). The survey and qualitative results revealed that girls tend to drop out of school at Form 4 (secondary school). Only 36% of the sample was attending school at the time, and many adolescent girls did not complete school due to lack of money for school fees, pregnancy, long distances to travel, household demands and migration for work (particularly among older adolescent girls). School attendance is primarily decided by parents, with some adolescent girls reporting that they make this decision themselves.
While most of the sample had never been married (97%), pregnancy was common (27%), with 89% of pregnancies being outside marriage. The average age at first marriage was 16.6 years (SD 1.2) (Table 1). Among those who had ever been married or ever been pregnant, 120 (61%) reported using a condom at last their sexual encounter. Many adolescent girls reported that their aunts were a major source of information on pregnancy and contraceptive use. Health facilities were the primary source of contraception obtained by adolescents, followed by shops/stores (where many adolescents were said to spend their free time). During FGDs with mothers, some reported that they helped ensure their daughters had access to family planning.
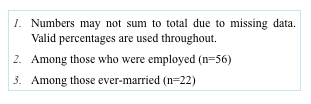
Of surveyed adolescent girls, 47% were food-insecure and 66% had poor dietary diversity, yet rates of stunting and thinness were under 10% (Table 2). Previous research has shown that menarche (or puberty) may be an opportunity for catch-up growth. Thus, we explored whether stunting was higher in those pre-menarche or post-menarche and found that of those adolescents who were pre-menarche, 17.7% were stunted (HAZ <-2 SD), while among those who were post-menarche, only 2.3% were stunted. The correlation between menarche and stunting was significant (p<.001), but should be interpreted with caution due to the smaller sample size.
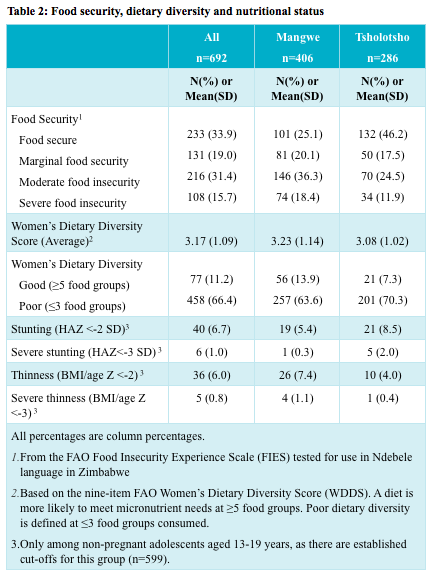
Comparing mean dietary diversity score across levels of food insecurity (Figure 3), we find that greater food insecurity is statistically significantly correlated with lower dietary diversity (Pearson X2 28.14, p<.001). This indicates food insecurity may be contributing to poor dietary diversity among adolescent girls.
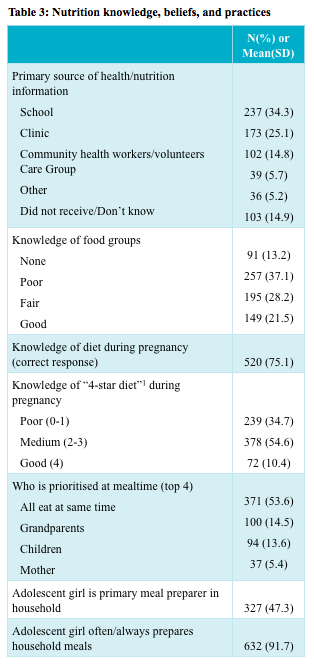
A variety of socio-behavioural factors were identified that may contribute to adolescent girl nutrition status (Table 3). Adolescent girls were commonly engaged in food preparation (92%), but had little food-related decision-making power. Mothers were the primary decision-makers surrounding both food purchases and preparation. Adolescent girls had low levels of knowledge on nutrition, particularly nutrition during pregnancy. Adolescent girls’ primary source of health/nutrition information was school (34%), followed by clinics (25%) and community health workers/volunteers (15%). Another 15% reported that they did not receive or did not know where they received health/nutrition information.
Only 14% of adolescent girl respondents could correctly identify the five critical handwashing moments; a risk factor for diarrhoea, infection and poor nutritional status. Most households where adolescents were residing get their water from a borehole and about 87% of adolescent girls are involved in fetching and carrying water regularly, with distances typically less than 30 minutes away, but sometimes reaching one to three hours of walking. Most girls reported being able to bathe more often during menstruation and most had the products they needed to manage menstruation, although some were using found items such as old rags or leaves rather than sanitary products from a store.
Reported health-seeking was high, with 97% of adolescent girls saying they seek assistance when they are sick or have a health-related concern. Similarly, the majority (97.3%) said they feel comfortable seeking health services as an adolescent and that the services meet their needs. Among those who said they were uncomfortable (2.4%) or felt the health services did not meet their needs (2.7%), the following reasons were given: nurse attitude (nurses were said to be ‘mean’, aloof, rude, or accused the girls of ‘loose morals’), slow service/long lines, hesitancy to go accompanied by parents and lack of medications or corruption in distribution. While 43% of adolescent girls said they choose to seek healthcare for themselves, others pointed to their mother or grandmother as the primary decision-maker on their own health-seeking.
Discussion
This assessment identified a variety of socio-behavioural and other factors that may contribute to adolescent girl nutritional status and practices in Zimbabwe. Many experience food insecurity and related poor dietary diversity, indicating their diets are unlikely to meet micronutrient adequacy (although stunting and underweight were found to be under 10%). The overall women’s dietary diversity score for adolescent girls in our sample was 3.2, which is similar to the dietary diversity score (3.1) found in a recent Title II Food for Peace baseline survey among the population in Amalima and ENSURE programme areas (USAID, 2015).
Pregnancy among unmarried adolescent girls is common, with low contraception use, indicating more work is needed to increase both knowledge and use of contraception for delaying pregnancy and practicing safe birth-spacing. Due to heightened nutritional needs in this age group, pregnancy poses additional risks for adolescent girls and their babies. In addition, although about 60% of married/sexually active adolescent girls reported condom use at last sexual encounter, continued promotion of condom use for protection against sexually transmitted infections is important, particularly given that the HIV prevalence rate in Zimbabwe is 15.2% (Zimbabwe Demographic Health Survey, 2010-11).
A variety of ‘key influencers’ or ‘gatekeepers’ were identified. As mentioned, the aunt was identified as a major source of information for adolescent girls on pregnancy and contraceptive use, and may have influence over nutrition or food-related decisions, depending on household structure. The mother was identified as the primary decision-maker surrounding both food purchases and food preparation. Adolescent girls commonly decide for themselves about seeking health services, and many identified their mothers or grandmothers as key influencers in health-seeking decisions. Decision-making on school attendance is made primarily by parents, with some adolescent girls reporting they make this decision themselves, which indicates a need to involve parents in any programmes intending to incentivise adolescent girl school attendance.
Recommendations
A key recommendation is to provide integrated behaviour change activities on sexual and reproductive health, WASH and nutrition through platforms where adolescent girls spend time: school clubs, sports, care groups, religious gatherings and water collection points.
Interventions to keep older adolescent girls in school while promoting improved diets and delayed pregnancy/marriage are critical, potentially including peer-to-peer models, incentives (e.g. income-generating activities contingent on school attendance, take-home food rations, etc.), community conversations among ‘key influencers’, and mobile phone messaging.
Men and boys should be engaged in efforts to reduce and delay adolescent pregnancies. Based on qualitative findings, several groups of men and boys stood out as key groups to target in reducing adolescent pregnancy. These include: cattle herders, local non-school-going adolescent boys and men returning home during the holidays from cross-border work. Although we did not interview husbands of adolescent girls, this group should be considered as well. Working with these populations to ensure they have both contraception knowledge and access to contraceptives may help prevent adolescent pregnancy.
Finally, programmes and policies addressing food insecurity alongside ongoing nutritional surveillance among adolescent girls are critical, due to the very high rates of food insecurity. This could include working with the private sector (such as input dealers, seed dealers, etc.) to improve access to nutrient-rich local foods and/or providing cash vouchers to give users flexibility to access needed commodities, depending on markets.
This assessment highlights the gap in knowledge on adolescent girl nutrition in Zimbabwe and provides some insight on what programming priorities should focus upon. However, further research is needed, including: assessment in other provinces or at the national level; further assessment to confirm adolescent use of health service across Zimbabwe; research on the nutritional value of indigenous/traditional foods and adolescent preferences; measurement of anaemia status; follow-up research on men’s perspectives and roles/behaviours to determine best approaches to engage adolescent boys and men to prevent unplanned/early pregnancy; and general research to establish age-appropriate cut-offs for measurement of adolescent girl nutritional status. Additionally, global gaps in knowledge on adolescent nutrition remain. Particularly of relevance to this assessment was lack of evidence to inform guidance on mid-upper arm circumference (MUAC) cut-offs for pregnant adolescent girls, as well as the need for more appropriate adolescent reference populations by region or country to enable more accurate calculation of adolescent nutritional status.
For more information, contact: Amelia Reese-Masterson
References
Reese-Masterson A, Murakwani P & Mlobane Z, 2015. Assessment of Adolescent Girl Nutrition, Dietary Practices, and Role in Zimbabwe: Mangwe and Tsholotsho Districts. June 2015. International Medical Corps.
USAID 2015. Baseline Study of Title II Development Food Assistance Programs in Zimbabwe, 2015.
Zimbabwe Demographic Health Survey, 2010-11.