
WHO emergency nutrition response in South Sudan
By Marina Adrianopoli and Allan Mpairwe
Marina Adrianopoli has been supporting WHO in South Sudan as Emergency Nutrition Focal Point since 2014. She has over 10 years’ experience in advising on and implementing nutrition emergency response, policy-making processes and country-level programmes focusing on public health nutrition and food and nutrition security in different emergency and development contexts in East Africa, Central Asia and Eastern Europe.
Dr Allan Mpairwe is the Programme Manager for Health Security and Emergencies for the WHO Country Office in South Sudan. He has over 15 years’ experience in implementing emergency health services in resource-limited settings and has supported emergency response operations in South Sudan for the last seven years. He was instrumental in the initiation and introduction of the new kit for management of children with SAM with medical complications in South Sudan.
The authors gratefully acknowledge Dr Usman Abdulmumini, WHO Representative in South Sudan, and colleagues from the Country Office in Juba, Magda Armah, Health Cluster coordinator, and Sylvain Denaire, Operation Officer, for playing a crucial role in supporting the implementation process at the national level. Thanks also to Havaskhon Abdulatipova, Henry Lagu and the staff of the WHO Juba Logistics Unit, who provided logistics support. Deep appreciation is expressed to Dr Adelheid Onyango, WHO AFRO Regional Advisor for Nutrition, Sophie Laroche, WHO HQ Essential Medicines, and colleagues at WHO Headquarters Department of Nutrition for Health and Development for their technical guidance, advice and continued support.
A poster sharing these experiences was presented at the World Nutrition Congress, Cape Town, South Africa, in September 2016. Improving strategies for inpatient management of severe acute malnutrition and medical complications in children: A new WHO medical module distributed in South Sudan as innovative WHO Emergency Response on Nutrition. Marina Adrianopoli, Allan Mpairwe and Sophie Laroche.
Location: South Sudan.
What we know: Management of SAM children with medical complications is critical; communicable disease burden can rise in emergencies, increasing caseload and adding strain to existing health services, including key medicines supply and management.
What this article adds: Throughout the heightened emergency phase in South Sudan from 2014 to 2016, WHO intensified support to nutrition programmes with increasing focus on inpatient management of medically complicated severe acute malnutrition (SAM). A SAM-specific medicines kit was devised and introduced in June 2016, along with a comprehensive capacity-building package and consistent M&E tools, in line with existing WHO Global Guidelines and national information systems of the health and nutrition sectors. Kits were distributed to one third of functioning stabilisation centres before the latest escalation in violence disrupted services and monitoring. This initiative reflects WHO’s operational role in nutrition programming in emergencies.
Context
Current crisis
South Sudan, the world’s newest nation, has chronic vulnerabilities and is faced with multiple crises alongside historical marginalisation, acute insecurity, economic decline, disease and lack of access to services, infrastructure and food. The armed conflict in South Sudan has caused a major public health crisis since December 2013, disrupting essential primary and secondary healthcare services and infrastructure. Since then, despite diminishing intensity of the armed violence and increased humanitarian access in the most-affected areas, the conflict has spread to new areas that were previously stable, causing further displacement and damage to livelihoods. In July 2016, the country was already facing rising food insecurity (due to deepening economic crisis, unresolved tensions and depleted food stocks from limited household production) and critical malnutrition levels, when renewed and severe conflict broke out. This has sparked a new wave of mass displacement and has been devastating for civilians; health and nutrition facilities have been attacked, damaged and looted.
Prior to the July 2016 crisis, 4.42 million people were estimated to be in need of emergency healthcare; an estimated 4.7 million people are now in need of health assistance. The conflict has compounded an already dire health situation, documented by appalling health indicators, including the following mortality rates: maternal (2,054/100,000 live births); neonatal (43/1,000); infant (83/1,000); and under-fives (106/1,000).
The current prevalence of acute malnutrition in South Sudan is unprecedented. Global acute malnutrition (GAM) rates now exceed emergency thresholds of 15% in all states except Central Equatorial and Lakes. An estimated 5.1 million people are classified as severely food and nutritionally insecure. The GAM level in Northern Bahr el Ghazal, one of the 10 former states of South Sudan before reorganisation in 2015, has hit the catastrophic level of 33.3%, indicating that one in every three children aged 6 to 59 months is acutely malnourished. In Western Bahr el Ghazal, GAM prevalence is now 20.6%, a nearly two and a half-fold increase in malnutrition in the last six months (8.5%, Dec 2015). Food insecurity is at critical levels in Northern Bahr el Ghazal, Warrap, Western Bahr el Ghazal, Upper Nile, and Lakes Region.1
WHO role in South Sudan
Less than 40 per cent of the population has access to basic health and humanitarian services, and more than one third is in urgent need of food, agriculture and nutrition assistance. The WHO Country Office (WCO) in South Sudan provides basic healthcare in line with the WHO/AFRO transformation agenda 2 and Universal Health Coverage principles. Adequate and timely health humanitarian response and surveillance are effected through coordination with partners, addressing inequality in the delivery of priority health services across the country by targeting the most under-served populations. As Health Cluster lead agency, WHO works to ensure a functioning health sector coordinating mechanism involving UN agencies, partners, health authorities, donors and community members, and provides up-to-date information on country health situation and needs, including regular situation reports and bulletins.3
Under the Health Security and Emergencies operations, emergency nutrition is a strategic sector for WHO in South Sudan. Since the onset of the crisis in early 2014, WHO has provided technical and strategic guidance to the nutrition humanitarian community and Ministry of Health (MoH) during the level 3 emergency. It has effectively supported review of strategic plans, policies, guidelines and criteria, and provided operational guidance on nutrition, through close collaboration with the MoH and partners. WHO is also actively engaged in intensifying timely sharing of nutrition information to better plan the response, as well as strengthening linkages and integration between health and nutrition.
This article documents WHO-led developments and progress around the treatment of complicated SAM in South Sudan.
Identified gap: Challenges in management of complicated SAM
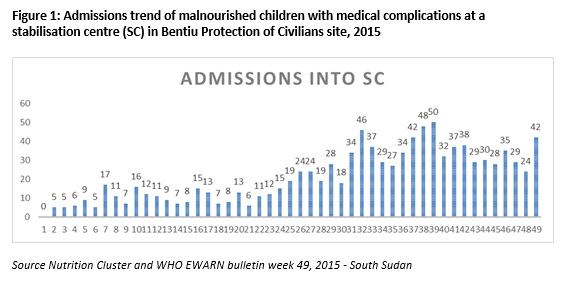
According to Nutrition Cluster (NC) projections, in 2016 nearly 690,000 children under five years of age are expected to be acutely malnourished, of whom more than 230,000 will be severely malnourished. The burden of SAM children with medical complications is significant and estimated at up to 10% of the total SAM caseload (approximately 6% in 2015).4 Figure 1 reflects the admissions trend of malnourished children with medical complications at a stabilisation centre (SC) through 2015. Medical complications of SAM include: severe oedema; poor appetite including inability to suckle breastmilk effectively; and one or more Integrated Management of Childhood Illness (IMCI) danger signs.5 Children presenting these conditions should be treated as inpatients in SCs, where clinical and nutrition care is provided. However, the lack of basic medical supplies drastically reduces the capacity to deliver effective and immediate response.
The most common morbidities amongst internally displaced persons (IDPs) in South Sudan are acute respiratory infection (ARI), acute bloody diarrhoea, and malaria (see Table 1); the most common causes of death are malaria, followed by ARIs, and acute watery diarrhoea. Communicable diseases remain a concern throughout the country due to poor sanitation, shortage of safe drinking water, crowded living conditions, malnutrition, and poor immunity. There has been a notable upsurge in the scale and frequency of outbreaks of epidemic-prone diseases, especially in displacement sites where malnutrition and poor immunity render young children and pregnant women particularly vulnerable. A major cholera outbreak was reported in the second quarter of 2016 and is ongoing.
Table 2. Top causes of morbidity among IDPs6
As of September 2015, some 55% of the health facilities in Unity State, Upper Nile State and Jonglei were no longer functioning. Stock-outs of essential medicines exacerbate the critical situation.7 The conflict hampers access to and delivery of humanitarian assistance and has already increased the operational costs of implementing the humanitarian response. This is exacerbated by the very fragile health systems (lack of skilled staff, supplies and equipment, leadership, functioning facilities, etc.) at all levels. Most of the health facilities in Juba and affected states are almost non-functional, as health personnel fail to report for duty due to the prevailing insecurity.8 SCs are usually set up in hospitals or in Primary Health Care Centres (PHCCs), which are normally situated at Payam headquarters. They provide referral services as well as laboratory services for diagnosis, maternity and inpatient care. Each PHCC is expected to serve a catchment area of around 50,000 people. Drugs used in the SC are part of the hospital or PHCC package; therefore SCs rely on hospital and PHCC stock and use medicines that are also administered to sick non-SAM children who present. As a result of service integration, procurement and budgeting exclusively for SCs’ stock of medicines is not common practice. Since they are embedded in static health facilities, SCs are also more exposed to closure in times of insecurity and displacement compared to outreach and outpatient mobile nutrition services.
WHO response
An improved inpatient care component of CMAM in South Sudan called for measures to address critical drugs shortage through timely procurement of essential medicines, ensuring coverage countrywide including conflict-affected areas and in terms of protection of civilians (PoC). Additional actions such as training were required to develop and reinforce the capacity of medical teams managing patients with SAM with medical conditions. In this challenging context, WHO South Sudan has identified the provision of a medical kit for SCs and the related capacity-building package and guidelines as a comprehensive strategy to support SCs managing SAM children with medical complications (MSAM/MC).
The innovative procurement strategy shaped by WHO in South Sudan entails:
- Design and technical development of an innovative kit (see Box 1), which has been distributed in South Sudan and has been available in the online WHO catalogue since April 2016. South Sudan was the first country in the world to introduce the medical kit in June 2016;
- Standardisation of the set of medicines needed in SCs, aligned to South Sudan national medicine usage and taking into consideration quality, safety and efficacy of medicines supplied;
- Fast track procurement, involving supply of standard, pre-packed kits ready to meet priority health needs in an emergency, agile supply chain management and strategic sourcing of SC drugs to support positioning of supplies;
- The inpatient care component of the Integrated Management of Acute Malnutrition (IMAM) national guidelines will be updated, aligned with the Hospital Care of Children Pocket Book 2013 (reference guidelines in SCs);
- Quality assurance, as all drugs are obtained from reliable sources; and
- Integrated feedback mechanism (report), so that the service can be continuously improved in response to feedback on delivery.
This strategy enables MoH and partners operating SCs to be autonomous in providing timely treatment. It also provides a stopgap measure, offering relief for hospital stocks of medicines, which currently are not procured and managed specifically for children with SAM/MC.
Training
To provide guidance on medicine usage and support partners in delivering refresher training to staff working in SCs, WCO South Sudan has developed a context-specific, capacity-building package on inpatient management of SAM focused on medical conditions. Building on the WHO Guidelines and training for the inpatient treatment of severely malnourished children9, the package has been developed by WHO Emergency Nutrition South Sudan, with the support of implementing partners and WHO AFRO Regional Office, and cleared by MoH, Republic of South Sudan.
The package consists of four tools:
1) A comprehensive refresher training of 70 slides covering key steps of the Management of SAM/MC, addressing both clinical and supportive care for conditions to be treated with the medicines provided. Most slides can be used as stand-alone handouts or posters. It is not a substitute for full training on appropriate management of SAM with medical complications, designed for healthcare providers.
2) A pictorial manual illustrating medical conditions associated with SAM in children, accompanied by detailed explanations.
3) Pocket book of hospital care for children: Second Edition – Guidelines for the management of common childhood illnesses. This includes a full chapter on the inpatient management of SAM, web link to the Pocket book10 and links to free applications for android phones and iphones.
4) WHO video – Emergency Treatment, which illustrates urgent actions required and standard emergency procedures on giving oxygen, glucose, fluid and antibiotics to help improving the quality of inpatient care for the management of SAM/MC in children.
The capacity-building package was illustrated to the nutrition and health community in South Sudan during the ‘kick off’ meeting and distributed to all nutrition and health cluster partners running inpatient care programmes. Technical orientation on the package has been provided by WHO during ad hoc orientation sessions conducted collectively and on a one-to-one basis with all interested partners and the MoH.
Box 1: Content of WHO SAM kit
The objective of the new WHO kit Second line drugs for the medical management of Severe Acute Malnutrition with medical complications is to provide essential drugs for the inpatient management of severe acute malnutrition with medical complications in children (MSAM/MC).
The content is organised into four modules which constitute one kit, sufficient to treat 50 children with SAM/MC. The kit contains 33 medicines and 11 health commodities. The modules are:
ROUTINE DRUGS MODULE
Contains routine drugs also used in outpatient nutrition programmes (anthelminthic, antibiotics, retinol and resomal).
BASIC MODULE (analgesic, antifungal, antibiotics, solutions for treatment of hypoglycaemia, dermatological preparations, ophthalmological preparations, health commodities and renewable).
SUPPLEMENTARY MODULE (medicines used in heart failure, antibiotics, ophthalmological preparations).
MALARIA MODULE (Coartem tablets, artesunate, malaria rapid diagnostic tests and lancets), incorporated in the kit to address one of the top priority diseases reported in the context under consideration.
The kit does not contain nutritional commodities as it has been designed to complement existing kits, equipment and supplies already provided by UNICEF and WFP. The provision of kits complements the collective NC response in South Sudan, largely focused on outpatient and preventive care of SAM.
The kit was established in line with the recommendations of the 1999 WHO Management of severe malnutrition: a manual for physicians and other senior health workers and the Course Director Guide of the related WHO Training Course, 2002. The list of drugs, initially developed in 2011, was reviewed by SAM management experts, the WHO Expert Committee on Essential Medicines, and with advice from colleagues from relevant WHO departments (HAC, CAH), and revised accordingly.
Monitoring
Five monitoring components have been developed by WHO South Sudan aimed at collecting, managing, analysing and reporting on key indicators to track progress, plan response and prioritise actions to improve service delivery (see Box 2).
Box 2: Monitoring tool
Tool 1: Stock inventory form, to track the quantity of medicines dispensed and the balance in each facility.
Tool 2: The Inpatient Therapeutic Programme (ITP) SC data collection form, employed by the current Nutrition Information System (NIS) of the NC in South Sudan, is integrated as the second tool. Partners are required to continue reporting to the NC on a monthly basis, as per the established mechanism; WHO has supported the NC in advocating for an increased reporting performance.
Tool 3: Additional information on the medical conditions diagnosed and treated, including eye problems, severe anaemia, SAM with oedema, malaria, suspected/confirmed HIV infection and ARI (including TB and pneumonia).
Tool 4: Final feedback form, to assess the appropriateness of medicines and material provided (quantity, suitability) and suggestions for improvements.
Tool 5: Challenges and strengths, for submission at least once and any time during implementation.
Preparatory work
A consultative process began in November 2015 led by WCO Emergency Unit/Nutrition, involving the MoH, NC, Health Cluster and implementing partners, and technically supported by WHO HQ. Key steps of the process have included technical consultations with MoH Pharmaceutical Department, Nutrition Unit and Primary Director General; verification and review of the list of medicines to ensure consistency with the List of Essential Medicines of South Sudan; and meetings with partners at different levels to corroborate the effectiveness of drugs utilisation. This information, together with several field-mission findings, was instrumental in better identifying capacity needs, information gaps, stock capacity and skills in management of supplies. This laid the foundations for developing the capacity-building and monitoring packages.
Implementation
Procurement of the first 20 kits by WHO South Sudan began in November 2015. The process of procurement for these initial kits was long (six months) as it involved medicine procurement from different suppliers, MoH clearance and assembly of the kits in Juba. (Now that the kit features in the WHO online catalogue, the shipment takes approximately one month from the purchase order). The first recipient, MoH, and partners’ facilities were selected based on average monthly caseload, prevalence of GAM (and associated SAM) in the catchment area, population figures including number of children under five as per the official statistics, documented gaps in stock of medicines, and confirmed presence of medical officers operating in the SC (given the nature of the kit and skillset required). The selection process was coordinated by WHO Emergency Nutrition, supported by the Health and Nutrition Cluster coordination team and guided by the MoH.
The strategy was launched in June 2016 in conjunction with the distribution of kits. The distribution covered nearly one-third of the total functioning SCs across all ten (former) states (16 facilities out of a total 58 11, ranging from hospitals to PHCCs in host communities, IDP and PoC sites. Supplies are calculated to treat 1,000 children over three months. The distribution strategy took into account the different levels of vulnerability across the country and aimed at responding to the high needs in urban contexts and PoC sites, where the SCs integrated in the main hospitals of the capital Juba and clinics in PoC sites required increased support.
Sadly, as soon as the distribution was completed, a renewed and terrible wave of violence erupted again, drastically reducing the capacity of partners to respond to the emergency. Most of the staff were relocated (WHO and other nutrition/health cluster implementing partners’ personnel worked remotely from the region in July, August and September) and the monitoring system has been interrupted.
Conclusions
The overall response reflects an active implementing role of WHO in an emergency, specifically in the context of the CMAM approach. WHO’s role has been to strengthen complicated case management, which tends not to attract the same attention as the prevention, outreach and outpatient services for MAM and SAM children. The experience in South Sudan reflects efforts to strengthen coordination and synergies between clusters and other key actors at national and field levels in the context of CMAM. The development of a standardised module of medicines for SAM/MC brought a unique opportunity for WHO South Sudan to increase effectiveness and sustainability of life-saving nutrition interventions and to boost WHO strategy shaped around improved inpatient management of SAM/MC, which encompasses provision of medical supplies, capacity-building and review of national guidelines.
For more information, contact: Marina Adrianopoli, email: Marina.adrianopoli@gmail.com, tel: +393497507123 or Dr Allan Mpairwe, email: mpairwea@who.int ; ampairwe@gmail.com, tel: +256772510026.
1 IPC analysis 2016.
3 The work of WHO in South Sudan, 2015. Working towards better health outcomes for the people of South Sudan.
4 South Sudan Humanitarian Response Plan 2016.
5 www.who.int/maternal_child_adolescent/documents/IMCI_chartbooklet/en/
6 WHO South Sudan (EWARN) Early warning and disease surveillance bulletin. www.who.int/hac/crises/ssd/epi/en/
7 WHO/MOH Situation Reports on Cholera in South Sudan, August 2016.
8 Humanitarian Needs Overview, 2016.
9 Based on WHO Guidelines for the inpatient treatment of severely malnourished children, available at www.who.int/nutrition/publications/severemalnutrition/9241546093/en/, and WHO Paediatric emergency triage, assessment and treatment: care of critically-ill children Updated guideline 2016 www.who.int/maternal_child_adolescent/documents/paediatric-emergency-triage-update/en/
10WHO Pocket book of hospital care for children: Second edition www.who.int/maternal_child_adolescent/documents/child_hospital_care/en/
11Nutrition Cluster, March 2016.