
Mortality and causes of mortality in children 6-59 months of age admitted to inpatient therapeutic feeding centres in Niger
By Florence Tapié de Céleyran, Kerstin Hanson, Cecilia Ferreyra, Nuria Salse, Didier Tshialala, Cristian Casademont, Rebecca Grais and Helena Huerga
Florence Tapié de Céleyran is a Clinical Epidemiologist with Epicentre, Paris
Kerstin Hanson is Paediatric/Nutrition Adviser with Médecins Sans Frontières (MSF), France
Cecilia Ferreyra is HIV/TB Adviser with MSF Spain
Nuria Salse is Nutrition Adviser with MSF Spain
Didier Tshialala is a Medical Doctor with MSF Spain
Cristian Casademont is Head of the Operational Medical Unit, MSF Spain
Rebecca Grais is Director of Research at Epicentre, Paris
Helena Huerga is a Clinical Epidemiologist with Epicentre, Paris
We would like to thank the staff of Koutiala, Madarounfa and Madaoua Therapeutic Feeding Centres for their work. Special thanks to Seybou Diarra and Abou Coulibaly from Koutiala Hospital and Yazi Abdoulaziz from Madarounfa Hospital. We are grateful to the Médecins Sans Frontières teams in Niger and Mali and the Epicentre team in Niger for their support and for making this study possible.
Location: Niger
What we know: Children with severe acute malnutrition with medical complications are at heightened risk of death.
What this article adds: Médecins Sans Frontières (MSF) examined mortality, causes of mortality and co-morbidities among children aged 6-59 months admitted to an inpatient therapeutic feeding centre (ITFC) in three MSF-supported sites in Niger, for all cases and for poor responders to treatment. A total of 2,765 children were included in the study. The principle cause of morbidity in all three sites was malaria (30-61.3%). The leading causes of mortality were sepsis, malaria and respiratory infection. Higher proportional mortality due to malaria in one site was likely seasonal. Poor response to ITFC therapy varied between sites (4.6-23.6%). Leading causes of mortality (ranging from 4.3 to 8.8%) among poor responders were: malaria, diarrhoea, sepsis, respiratory infection (including TB) and HIV. HIV prevalence in one site was 5.4% on selective screening and 0.5% on post-study systematic screening. Respiratory infection was an important cause of mortality in all sites; case detection and case fatality for TB was likely under-diagnosed.
Background
 Malnutrition is responsible for nearly half (45%) of all deaths in children under five years old (Black et al, 2013). Current guidelines recommend that children with severe acute malnutrition (SAM) and medical complications or poor anthropometric or clinical improvement after two or three weeks of nutritional and medical therapy in an Ambulatory Therapeutic Feeding Centre (ATFC), be referred to an Inpatient Therapeutic Feeding Centre (ITFC) for specialised treatment and further medical evaluation and investigation (WHO, 2013[1]; WHO, 2013[2]; MSF, 2016). Médecins Sans Frontières (MSF) examined mortality, causes of mortality and co-morbidities among children under five years of age admitted to an ITFC in three sites in Niger, for all cases and for poor responders to standard ITFC therapy.
Malnutrition is responsible for nearly half (45%) of all deaths in children under five years old (Black et al, 2013). Current guidelines recommend that children with severe acute malnutrition (SAM) and medical complications or poor anthropometric or clinical improvement after two or three weeks of nutritional and medical therapy in an Ambulatory Therapeutic Feeding Centre (ATFC), be referred to an Inpatient Therapeutic Feeding Centre (ITFC) for specialised treatment and further medical evaluation and investigation (WHO, 2013[1]; WHO, 2013[2]; MSF, 2016). Médecins Sans Frontières (MSF) examined mortality, causes of mortality and co-morbidities among children under five years of age admitted to an ITFC in three sites in Niger, for all cases and for poor responders to standard ITFC therapy.
Methods
This was a prospective study that included all children aged 6-59 months with SAM hospitalised in the ITFCs of Koutiala (Mali), Madarounfa (Niger) and Madaoua (Niger). All three sites were supported by MSF. SAM was defined by a weight-for-height z-score (WHZ) < −3 and/or mid-upper arm circumference (MUAC) < 11.5 cm and/or bipedal oedema (WHO, 2013[2]).
Poor response to ITFC therapy was defined as follows:
- In Koutiala and Madarounfa (MSF definition) – Stagnating weight or persistence of oedema or poor clinical evolution two weeks after admission, regardless of the clinical/anthropometric evolution prior to admission;
- In Madaoua (Niger National protocol definition) – Children with one of the following criteria: Clinical deterioration at any time after admission; failure to improve/regain appetite by Day 4; failure to start to lose oedema by Day 4; presence of oedema at Day 10; failure to fulfil criteria for discharge towards an ATFC by Day 12; stagnant weight for two to three weeks before admission.
Causes of mortality were the clinical diagnoses given by the on-call physician at time of death. Causes of morbidity were those identified during routine daily care and classified as primary and secondary causes of morbidity (at time of exit from the hospital). The analyses of causes of mortality and morbidity took only primary diagnoses into account.
Routine data from the medical files of the patients were collected using a standard form. Data were entered in an Epidata database and analysed using Stata 13.
Results
In total, 2,765 children were included in the study: 1,337 children in Koutiala and 437 in Madarounfa (from 19 November 2014 to 18 February 2015) and 991 children in Madaoua (from 15 September to 14 December 2014). The sex ratio was around 1:1 in all three sites. Median age varied from 14 (IQR: 9-24) months in Madaoua to 24 (IQR: 12-24) months in Koutiala. Median length of stay was four to five days in all three sites.
Almost half of the admitted children were transferred from ATFCs. In Koutiala, 18% were admitted because of lack of response to treatment, whereas in Nigerien sites this applied to a smaller proportion of admissions (1.8% in Madarounfa and 8.8% in Madaoua). The evolution during hospitalisation was favourable for 90 to 94% of our study population. The inpatient mortality rates observed were 6.4%, 7.8% and 5.2% in Koutiala, Madarounfa and Madaoua respectively. The proportion of defaulters was 0.2%, 0.2% and 0.5% respectively.
The principle cause of morbidity was malaria: 30.0% in Koutiala, 61.3% in Madarounfa and 55.0% in Madaoua. Rapid diagnostic tests were done systematically at time of admission in all three sites. In all locations, Plasmodium falciparum is prevalent and no drug resistance has been described. The second and third leading causes of morbidity were: respiratory infection (9.3%) and anaemia (8.2%) in Koutiala; respiratory infection (8.9%) and sepsis (8.0%) in Madarounfa; and diarrhoea (26.6%) and respiratory infection (8.1%) in Madaoua.
HIV testing in cases where HIV was suspected was undertaken in Koutiala and well accepted.1 HIV testing was not being performed in Madarounfa or Madaoua at the time of the study. In Koutiala, 11% of admitted children were tested based on clinical suspicion, among whom 8/149 (5.4%) were diagnosed as positive and started on treatment. Subsequently, in 2015, systematic HIV testing was implemented in Madaoua; around 0.5% of hospitalised malnourished children tested positive. Efforts have also improved in Koutiala, where nearly 50% of ITFC admissions were screened for HIV in 2016, with 1.9% (21/1,127) having a positive result. In Madarounfa, 36% of ITFC admissions were screened in 2016, with 1.9% (69/3,547) having a positive result.
The three leading causes of mortality were sepsis, malaria and respiratory infection (Table 1). In Koutiala, sepsis accounted for 43.0% of deaths, malaria for 15.1% and respiratory infection for 10.5%. In Madarounfa, 70.6% of the deaths were linked to sepsis, 17.7% to malaria and 2.9% to respiratory infection, while in Madaoua malaria was the principle cause (64.7%), followed by sepsis (9.8%) and respiratory infection (7.8%). The highest case fatality rates (CFR) were for meningitis, sepsis, hypovolemic shock, HIV and tuberculosis (TB).
Poor response to ITFC therapy was found in 7.6%, 4.6% and 23.6% of the study population in Koutiala, Madarounfa and Madaoua respectively (the wider definition of the Nigerien national protocol was used in the latter site). Mortality among poor responders was 8.8%, 5.0% and 4.3% in Koutiala, Madarounfa and Madaoua respectively. The leading causes of mortality among poor responders were: malaria, diarrhoea, sepsis, respiratory infection (including TB) and HIV.
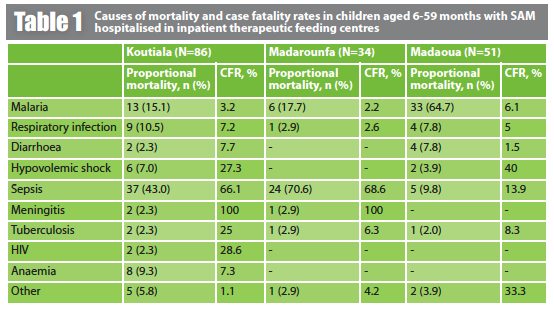
CFR: case fatality rate
Discussion
Mortality in children aged 6-59 months with SAM hospitalised in the three ITFCs was moderate when compared to international standards (5% to 10%) (Black et al, 2013) and lower than the mortality rates seen in other series (Ahmed et al, 2014; Patel et al, 2010; Page et al, 2013; Mahgoub & Adam, 2012; Dubray et al, 2008; Prudhon et al, 1997; Pécoul et al, 1992). Main causes of mortality: sepsis, malaria and respiratory infections, were similar to previous publications (Page et al, 2013; Mahgoub & Adam, 2012).
The higher proportional mortality due to malaria in Madaoua is probably linked to the timing of the malaria season in this site during the study period. Differences in the proportional mortality by site may also be due to reporting, as only the primary cause of mortality is taken into account in this analysis. Cause of death for cases with unclear diagnosis or with several concomitant pathologies may have been reported differently in the three sites. A large number of these cases may have been diagnosed as sepsis, particularly in Madarounfa and Koutiala.
Respiratory infection was an important cause of mortality in all sites and TB was described as the primary cause of death in a few of patients. Case fatality rates were particularly high for TB, probably due to delayed diagnosis. Due to the difficulties in diagnosing TB in malnourished children (lack of diagnostic tools and difficulties for children in producing sputum samples), some patients with TB may have been diagnosed and treated as having a respiratory infection of other origin.
Finally, in Koutiala, where a considerable number of children with SAM were selectively screened for HIV, a significant proportion were diagnosed as positive, compared to the adult prevalence rate in Mali (1.3% in 2015) (UNAIDS, 2015). However, post-study programmatic data from the three sites showed a lower HIV rate among hospitalised, malnourished children when HIV testing was systematic, particularly in Madaoua. HIV prevalence among hospitalised, malnourished children should therefore be locally assessed through HIV systematic testing in order to inform an HIV-testing strategy that might be different depending on the context.
For more information, contact: Helena Huerga, email: helena.huerga@epicentre.msf.org
Footnotes
1Rapid HIV tests were available on site and DNA Polymerase Chain Reaction (PCR) in the country capitals (three months delay in getting results).
References
Ahmed S, Ejaz K, Mehnaz A and Adil F. Implementing WHO feeding guidelines for inpatient management of malnourished children [Internet]. 2014. www.jcpsp.pk/archive/2014/Jul2014/11.pdf
Black RE et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, Volume 382, No. 9890, p427-451, 3 August 2013.
Dubray C, Ibrahim SA, Abdelmutalib M, Guerin PJ, Dantoine F, Belanger F, et al. Treatment of severe malnutrition with 2-day intramuscular ceftriaxone vs 5-day amoxicillin. Ann Trop Paediatr. 2008 Mar; 28 (1): 13–22.
Mahgoub HM & Adam I. Morbidity and mortality of severe malnutrition among Sudanese children in New Halfa Hospital, Eastern Sudan. Trans R Soc Trop Med Hyg. 2012 Jan; 106(1):66–8.
MSF, 2016. Me?decins Sans Frontie?res Clinical guidelines – Diagnosis and treatment manual. 2016 edition. ISBN 978-2-37585-001-5 [cited 2016 Nov 10]. refbooks.msf.org/msf_docs/en/clinical_guide/cg_en.pdf
Page A-L, de Rekeneire N, Sayadi S, Aberrane S, Janssens A-C, Rieux C et al. Infections in children admitted with complicated severe acute malnutrition in Niger. PloS One. 2013;8 (7):e68699.
Patel D, Gupta P, Shah D and Sethi K. Home-based rehabilitation of severely malnourished children in resource poor setting. Indian Pediatr. 2010 Aug; 47(8):694–701.
Pécoul B, Soutif C, Hounkpevi M and Ducos M. Efficacy of a therapeutic feeding centre evaluated during hospitalization and a follow-up period, Tahoua, Niger, 1987-1988. Ann Trop Paediatr. 1992; 12(1):47–54.
Prudhon C, Golden MH, Briend A and Mary JY. A model to standardise mortality of severely malnourished children using nutritional status on admission to therapeutic feeding centres. Eur J Clin Nutr. 1997 Nov; 51(11): 771–7.
UNAIDS. HIV and AIDS estimates [Internet]. 2015. [cited 2016 Dec 06]. www.unaids.org/en/regionscountries/countries/mali
WHO, 2013[1]. World Health Organization. Guidelines for the inpatient treatment of severe malnourished children. [Internet]. 2003 [cited 2013 Nov 30].
www.who.int/nutrition/publications/guide_inpatient_text.pdf
WHO, 2013[2]. World Health Organization. Guidelines Updates on the Management of Severe Acute Malnutrition in infants and children [Internet]. 2013 [cited 2014 Feb 20].
apps.who.int/iris/bitstream/10665/95584/1/9789241506328_eng.pdf