
Results and lessons learned from WFP’s efforts to support adolescent girls in Niger
By Alexandra Pirola, Benedict Tabiojong Mbeng and Mica Jenkins
Benedict Tabiojong Mbeng is Head of Nutrition for WFP Niger country office. He has over 30 years’ experience in nutrition programming and holds an MPH in Health Development from the Royal Tropical Institute (KIT) Amsterdam. He previously worked for WFP in Rwanda, Central Africa Republic (CAR) and Niger, as well as for UNICEF in CAR.
Alexandra Pirola worked as Programme Policy Officer in the Nutrition Unit of the World Food Programme (WFP) Niger Country Office between 2015 and 2017, focusing on nutrition and gender-sensitive issues. She holds an MSc in International Development and Humanitarian Emergencies from the London School of Economics (LSE).
Mica Jenkins is the Research and Evidence Officer for the Nutrition Division at WFP headquarters. She holds an MSc in Health and Human Development with a focus on nutrition and sustainable food systems. Prior to joining WFP, Mica implemented rural development and research projects in Mozambique and in the Dominican Republic.
Location: Niger
What we know: Adolescent pregnancy, associated with early marriage, greatly increases maternal and infant morbidity and mortality, has poor long-term outcomes, and fuels intergenerational malnutrition.
What this article adds: A World Food Programme pilot in Niger (2012-2015) targeted vulnerable adolescents with a joint education and nutrition programme delivered through primary and secondary schools. Daily meals for girls and boys in primary schools were fortified using micronutrient powders. Weekly iron and folic acid supplements were provided to secondary school girls and boys. A monthly scholarship was provided to girls to encourage school attendance, alongside community sensitisation. Anaemia prevalence significantly reduced in primary school boys and girls and secondary school boys, but not in secondary school girls. Nutrition knowledge, dietary diversity and consumption of iron-rich foods improved. The proportion of girls passing the school year doubled. An adapted, scaled-up version of the programme includes targeting education and support to poor and very poor households and a more intensive, girls-only supplementation protocol. Key lessons to date include the importance of national policy alignment, multi-stakeholder engagement, strong communication and the value of using existing platforms to improve programme delivery.
Background
Niger is a land-locked, low-income, food-insecure country in the Sahel that is highly exposed to climate change, ranking 187 out of 188 on the Human Development Index in 2016. Over two million people are food insecure and another 4.5 million are at risk of food insecurity, with millions more affected during the lean season. According to World Health Organization (WHO) classifications, Niger has a high global acute malnutrition (GAM) rate of 10% and very high stunting prevalence of 42% (WHO, 2018). An estimated 60% of school-age children in Niger do not consume sufficient vitamin A, with high anaemia levels affecting 75% of children under five years of age and 46% of women of reproductive age (EDSN-MICS, 2012).
There are gender disparities in the education system in Niger. According to UNICEF, school enrolment rates are 70% for boys and 57% for girls at primary level and 14% for boys and 10% for girls at secondary level. Girls’ access to education is limited by cultural practices, including responsibility for domestic chores and care for younger siblings, and structural factors, such as the scarcity of schools, resulting in long walking distances. An estimated 76% of adolescent girls in Niger are married before age 18 and one in four girls are married before age 15; this is one of the highest rates of early marriage globally. Early marriage correlates with high rates of adolescent pregnancy (48% of adolescent girls in Niger have a child before age 18), associated in turn with increased risk of maternal mortality, stillbirth, neonatal death, preterm birth and low birthweight (LBW) (EDSN-MICS, 2012).
Rationale for intervention
Maternal health and nutrition make major contributions to child health and nutrition throughout the life cycle (Black et al, 2008; Victoria et al, 2008). A malnourished woman is more likely to give birth to an LBW infant, increasing the risks of wasting, stunting and child mortality and, in adulthood, chronic diseases such as diabetes and hypertension. This vulnerability is passed from mother to child, perpetuating the intergenerational cycle of malnutrition. Adolescent girls are at high risk of anaemia, due to chronic iron depletion during the menstrual cycle; anaemia during pregnancy substantially increases the risk of LBW and maternal mortality. Interventions that aim to reduce anaemia prevalence among adolescent girls can therefore help reduce maternal mortality, LBW, child malnutrition and child mortality.
Parental schooling has been associated with improved child nutrition outcomes, including the reduction of stunting (Ruel et al, 2013). Formal education is also protective for girls, reducing the risk of exposure to abuse, early marriage and early pregnancies. Malnutrition negatively impacts education through reduced school attendance and achievements and, at the national level, reduces contribution to development in terms of human capital (Victoria et al, 2008). Interventions that combine keeping adolescent girls in the education system and their improved nutritional status can address these issues simultaneously to help break intergenerational cycles of poverty and malnutrition.

Designing and implementing the pilot
Between 2012 and 2015, the World Food Programme (WFP) Niger undertook a pilot project targeting vulnerable adolescent girls with a joint education and nutrition programme in Dogo, Gaffati and Koleram municipalities in Mirriah division of Zinder region, where school attendance was the lowest in the country. The project was implemented in 24 primary schools, reaching approximately 1,700 pupils in grades five and six (children aged 10 to15 years); of whom 48% were girls, and in six secondary schools, reaching approximately 1,400 students; 30% of whom were girls.
Unlike most WFP school meal programmes, the pilot targeted both primary and secondary students to encourage school attendance and performance, while simultaneously improving student nutrition knowledge and status. Additionally, gender-sensitive themes, such as the importance of girls’ education and dangers of early marriage, were discussed with both girls and boys. Children were encouraged to express their thoughts and ideas to improve confidence and self-esteem.
In collaboration with UNICEF, the nutrition component involved weekly iron and folic acid supplements for girls and boys in secondary schools during the entire school year from 2013 to 2015, according to WHO 2011 protocols (60 mg of elemental iron and 2.8 mg of folic acid once per week). For girls and boys in primary schools, daily meals were fortified using micronutrient powders (MNP). Deworming also occurred twice per year among primary school children, facilitated by the Ministry of Education.
The education component targeted girls in households categorised as poor and very poor using the household economy approach (HEA), with a monthly scholarship for two academic years (valued at USD7 per month) to facilitate and encourage school attendance. A total of 272 adolescent girls received the scholarship in the 2013-2014 academic year and 232 in 2014-2015. During the second year of the pilot, local committees were established to support and monitor the scholarship process in response to a recommendation from the mid-term review to improve girls’ school performance. Sensitisation sessions were also held in schools and at the community level, focusing on girls’ education, as well as essential family practices, hygiene, sanitation, nutrition and gender issues.
The total cost of the pilot phase was just under USD1.3 million, not including supplementation, which was in partnership with UNICEF.
Results of the pilot phase
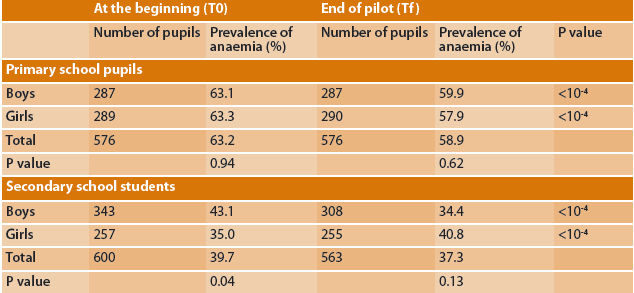
A significant reduction in anaemia prevalence was observed in targeted primary school children; from 63% to 58% for girls and 63% to 60% for boys. In secondary schools, anaemia rates among boys fell from 43% to 34% (see Table 1). Results also revealed that anaemia is predominantly mild1a> among affected boys and girls. No impact of iron and folic acid supplementation was observed among secondary school girls; in fact, anaemia rates increased from 35.0 to 40.8%. The team hypothesise that this is due to the impact of the initiation of menstruation. Also, boys tend to purchase meat-based snacks, while girls are more likely to purchase non-food items, leading to poor consumption of iron-rich foods.
Table 1: Anaemia prevalence at baseline and end of pilot project
Improved school results were observed among targeted secondary school girls; the percentage of girls who passed their school year increased from 32% (2013-14) to 68% (2014-2015). The local committees, composed of community members familiar with the local context and the challenges faced by adolescent girls, proved crucial in improving the percentage of girls who passed their school year from mid-way through the project.
Dietary diversity improved significantly among boys and girls in primary schools (boys from 60.6% to 78.6% and girls from 60.9% to 82.1%) and secondary schools (boys from 66.1% to 84.2% and girls from 70.8 to 81.6%), with notable increases in the percentage of all groups achieving high dietary diversity. The consumption of iron-rich foods also increased across all groups (primary school girls 34.3% to 48.6%; primary school boys 33.8% to 80.8%; and secondary school boy: 35.9% to 55%), with the exception of secondary school girls, whose consumption remained stable (42.0% to 42.6%). A questionnaire administered to both control and intervention groups revealed that nutrition knowledge also improved among boys and girls in primary and secondary school.
Sanitation and hygiene practices, though already shown to be strong at baseline, were endorsed and sustained by the intervention.
Scale-up and integration within the WFP Protracted Relief and Recovery Operation (PRRO)
WFP is currently implementing a protracted relief and recovery operation (PRRO) in Niger, aimed at strengthening household and community resilience through a countrywide, integrated, multi-sector and multi-partner safety net and disaster risk reduction approach. The PRRO is led by the Government of Niger in partnership with WFP, UNICEF, the Food and Agriculture Organization (FAO), the International Fund for Agricultural Development (IFAD) and other non-government organisations (NGOs).
Initiated in 2014, this intervention is based on an integrated package of activities, targeting the most vulnerable households. The package aims to help households build their resilience by targeting the different members as follows: screening and treatment of malnutrition for children under two years of age and pregnant women; information education and communication (IEC) on nutrition, DD, sanitation and hygiene for the whole household; school feeding for school-aged children; cash transfers, conditional on participation in the creation of productive assets activities; and unconditional cash transfers during the lean season. It is implemented in all seven regions (37 municipalities) of Niger.
The pilot was successful in improving the school attendance and performance and self-esteem of girls, as well as acceptance of iron-folic acid supplementation by the adolescents and the community members and knowledge on DD. The lack of impact on secondary school girls’ anaemia prevalence during the pilot indicated the need to increase the level of supplementation provided (in line with updated WHO recommendations) and provide more targeted sensitisation among girls to increase consumption of iron-rich foods and improve DD. A new cycle of the PRRO began in January 2017 which provided an opportunity to include an adapted and scaled-up version of the adolescent pilot project in the intervention strategy for all regions.
Adolescent girls between 10 and 19 years old from vulnerable households already receiving the integrated package of activities through the PRRO now receive targeted additional support to improve their school attendance and nutrition. An estimated 13,130 adolescent girls have been targeted with education grants through the programme and 50,636 adolescent girls have been targeted with iron-folic acid supplementation (around 0.5% of the adolescent girl population in Niger). Due to resource constraints and the special nutritional needs of adolescent girls, adolescent boys are not included in the scaled-up programme. Fortification of primary school meals with MNP was also discontinued to align with the newly established national strategy for school meals, which centres on ‘natural’ fortification through food combinations and improved DD.
Unlike the pilot, which targeted adolescents in schools for supplementation, the scaled-up programme provides supplementation to all girls aged between 10 and 19 years in target households, whether the recipient is the child of the head of the household or the adolescent wife/mother. This adaptation in the targeting strategy helps to ensure that girls out of school are also reached with nutrition support. In the scaled-up programme, supplementation has been increased to daily iron and folic acid supplements2 (containing 60mg iron and 400mcg folic acid), in line with updated WHO guidelines (WHO, 2016).
As in the pilot phase, girls receive a monthly scholarship of USD7 per month, intended to cover their basic needs and encourage them to pursue their studies. The scholarship is conditional on school attendance, which is monitored. Girls are supported by existing local committees, such as school management committees, parent-teacher associations, professors and local leaders, which ensure girls’ attendance and investigate reasons for absence, including living and studying conditions.
Gender-sensitisation and awareness-raising activities have been continued in the PRRO at the school and community levels, although these are now carried out by trained community animators rather than NGO staff to improve ownership and sustainability. Girls and boys, as well as community members, are sensitised on the importance and benefits of girls’ education and the risks of early marriage and early pregnancies. Adolescents are also supported in the development of life skills and educated on goal-setting and financial management (new since the pilot), thus further building their confidence and empowerment.
Programme adherence will be measured at midline and end-line points of the PRRO3. Two indicators will measure any reduction in incidence of anaemia: proportion of adolescent 10-19 year-olds in targeted households who received iron-folic acid supplementation for three successive months, and anaemia prevalence, measured through the Demographic and Health survey (DHIS) for 2017 and 2021 (regional/divisional DHS data will be examined). This activity is reinforced by nutrition education, with a specific focus on nutritional needs during adolescence, radio broadcasts and interpersonal communication at distribution sites. Sensitisation sessions are also held throughout the year in targeted primary and secondary schools.
Challenges, lessons learned and the way forward
Ensuring alignment with national policies and strategies is crucial for the uptake of the project and its sustainability
The intervention is aligned with the National Policy on Nutrition Security (2016-2025) and the National Multi-Sector Plan for Youth and Adolescent Health (2017-2021). These key documents include planned interventions that aim to reduce anaemia prevalence during adolescence through the distribution of iron and folic acid supplements and through sensitisation and communication for behavioural change around diet and food habits, scheduled to begin in 2018. The distribution of scholarships to girls is aligned with the priorities of the Education and Training Sector Plan (2014-2024), which aims to close the gender gap in education and support retention of girls in school.
Using established platforms and WFP presence helps new programme delivery
The integration of adolescent support within the WFP PRRO integrated package of activities helped maximise impact, given that communities were familiar with and trusted WFP, and existing platforms could be used. For instance, the distribution of iron and folic acid supplements to adolescent girls is a new intervention in Niger and stakeholders expressed concern about girls attending the distribution sites. Strong communication between project supervisors and beneficiaries before the distribution to address these challenges ensured that 90% of eligible girls received supplements during the 2017 lean season. Additionally, the distribution platform for general food distribution and screening and referral of malnourished children is now being used to distribute supplements, thereby reducing costs.
Interventions to target adolescents require the creation of an enabling education environment
An enabling environment is necessary to deliver a school-based nutrition programme. For example, the sensitisation of teachers on related themes ensured their interest and participation in project activities, encouraging sustainability of programme impact within the school and throughout the wider community. In many schools in Niger, as in many developing countries with high population growth, there is a huge demand for teachers and a lack of resources for teacher training beyond a very basic level. This reduces the overall quality of education. The high number of students also creates pressure on infrastructure and school resources, often resulting in inadequate classrooms and lack of classroom and teaching materials.
To face these challenges, WFP Niger focuses its interventions in ‘convergent municipalities’ – areas identified as the most vulnerable by the Government of Niger and where the United Nations System and the humanitarian community are requested to concentrate their efforts. Harmonisation and integration of activities is ensured in these areas through investment in schools for more teachers, improvement of the school environment (through provision of toilets, refectories and water supply) and teaching resources, thus creating an enabling educational environment to maximise the impact of WFP’s adolescentinterventions4.
Effective communication throughout the project cycle is essential for smooth implementation
During the pilot phase, several activities were implemented in schools by cooperating partners without the knowledge of the school authorities, decentralised education services, district health service or local health facilities. At times, these authorities were unaware of the activities taking place under the programme, or even the programme itself. This led to poor engagement and insufficient monitoring of these activities by the decentralised authorities, which reduced their acceptance and ownership of the intervention. Cooperating partners should therefore communicate effectively with school administration and all relevant stakeholders at the district and local level before organising any activity to take place in the school facilities to ensure that the benefits are understood, participation is maximised, and disruptions to school activities are avoided.
Adopting multi-partner approaches helps to strengthen efficiency and effectiveness
UNICEF was involved in design, implementation and monitoring during the pilot phase, as well as the design of the scaled-up programme, particularly the nutrition component (including supplementation) and communication strategy. Moving forward, WFP Niger plans to collaborate on programme implementation with various partners with complementary strengths, such as the UN Population Fund (UNFPA), the UN Entity for Gender Equality and the Empowerment of Women (UNWOMEN) and the UN Programme on HIV/AIDS (UNAIDS). Discussions are ongoing with these partners on the incorporation of HIV/AIDS awareness activities, gender awareness and adolescent-friendly areas in schools, and reproductive health activities.
Ensuring ownership at community, regional and national levels is key for project success
The project established partnerships with the Government through the relevant ministries (i.e. education and health) and through the Haut Commissariat à l’Initiative 3N (Les nigeriens nourrisent les nigeriens), also known as the 3N initiative. These stakeholders participate in the steering committee that provides technical advice and supervision. The full involvement of government representatives at national, regional and community levels is imperative for the success of the project. During the pilot phase, despite the high involvement of the national Government, decentralised regional and local authorities were not sufficiently involved in the design, implementation and monitoring, which resulted in a lack of ownership. With the scale-up effort, the full engagement of government counterparts at all levels was ensured by a series of visits in each region of implementation by the national monitoring committee, which held bilateral meetings with the relevant regional stakeholders to collect feedback. Regional committees were then established, in charge of closer supervision of the activities; these committees visited the local authorities to ensure their full involvement.
Conclusions
Good nutrition matters throughout the life cycle, but is especially important during the first 1,000 days of life when indisputable impacts on a child’s growth, learning and future productivity can be obtained. Compensating later in life for deprivations during this period is difficult, but possible during adolescence. To help break the intergenerational cycle of malnutrition, an integrated set of multi-sector interventions targeted at adolescents, which includes education and nutrition programming, is needed.
Lessons learned from the WFP pilot have shown that the active participation of communities – adolescent boys and girls, women and men – at all stages of the programme, as well as close coordination with government and other partners to improve delivery platforms, can help to remove barriers posed by access and socio-cultural norms which influence the good nutrition of adolescent girls in Niger.
For more information please contact Benedit Tabiojong or Mica Jenkins.
Endnotes
1Mild anaemia: Haemoglobin level for a child aged 5 to 11 years is 110-114 g/l and 110-119 g/l for children aged 12 to 15 years and above.
2Containing 30-60mg of elemental iron.
3It was not feasible to conduct baseline data collection due to the reopening of schools.
4These activities began in September 2017, therefore no evaluation of their impact has yet been conducted.
References
Black, R, et al. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet. 2008;371:243-60.
EDSN-MICS, 2102. Niger Demographic and Health Survey and Multiple Indicator Cluster Survey (EDSN-MICS) IV, 2012
Ruel, M, Alderman, H and the Maternal and Child Nutrition Study Group. Nutrition-sensitive interventions and programs: How can they help accelerate progress in improving maternal and child nutrition? Lancet. 2013;382(9891):536–551.
Victoria, CG, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340-57.
WHO, 2016. Guideline: Daily iron supplementation in adult women and adolescent girls. Geneva: World Health Organization; 2016.
WHO, 2018. Global Database on Child Growth and Malnutrition. Accessible at: www.who.int/nutgrowthdb/about/introduction/en/index5.html.