
Diet and nutrition status among school-age children and adolescents in Tanzania
By Sauli John, Geofrey Mchau, Heavenlight Ayubu, Stanslaus Mafung’a, Samafilan Ainan, Wiggins Kyatikila, Elizabeth Lyimo, Frank Chacky, Fatoumata Lankoande, Abraham Sanga, Pendael Machafuko, Ray Masumo, Ramadhani Noor, Kudakwashe Chimanya, and Germana Leyna
Sauli John is a nutritional epidemiologist and a public health specialist working with the Tanzania Food and Nutrition Centre (TFNC)
Geofrey Mchau is a principal epidemiologist with more than 14 years of experience at the Tanzania Food and Nutrition Centre
Heavenlight Ayubu is an assistant lecturer in Biostatistics and Head of Department at Muhimbili University of Health and Allied Sciences (MUHAS)
Stanslaus Mafung’a is a data scientist at the Ifakara Health Institute (IHI)
Samafilan Ainan is a Paediatrician and Researcher based at the National Institute for Medical Research in Tanzania
Wiggins Kyatikila is a statistician working as assistant lecturer at the University of Dar es Salaam College of Social Sciences, and Department of Statistics
Elizabeth Lyimo is a research officer working with the TFNC
Frank Chacky is the monitoring and evaluation specialist working with the Ministry of Health, Community Development, Gender, Elderly and Children through the National Malaria Control Programme in Tanzania
Fatoumata Lankoande is a nutrition specialist at UNICEF Tanzania
Abraham Sanga is a nutrition officer working with UNICEF Tanzania
Pendael Machafuko is a research scientist working with the National Institute for Medical Research in Tanzania
Ray Masumo is a director at the Department of Community Health and Nutrition at the TFNC
Ramadhani Noor is a nutrition specialist working with the UNICEF Tanzania country office
Kudakwashe Chimanya is a registered dietitian and nutrition specialist currently working with the UNICEF Tanzania office as the Chief of Nutrition
Germana Leyna is a managing director of the Tanzania Food and Nutrition Center.
The authors would like to thank all the individuals, institutions and partners who contributed to the data collection of the School Malaria and Nutrition Survey conducted in mainland Tanzania. Special gratitude goes to the Government of the United Republic of Tanzania, the Ministry of Health, Community Development, Gender, Elderly and Children, the President’s Office –Regional Administration and Local Government and the Ministry of Education, Science and Technology for their support to conduct this survey. We further acknowledge the Global Fund support on the implementation of the survey (design, orientation of field staff and data collection exercise), UNICEF for its technical and financial support, particularly on the nutrition aspect, and the U.S. President’s Malaria Initiative for providing financial and technical support on data management and report writing through RTI International.
Location: Tanzania
What this article is about: This article features a cross-sectional survey of 68,147 children (5-19 years of age) in Tanzania between August and October 2019 to assess nutritional status and dietary quality using anthropometry and dietary recall methods.
Key messages:
- The findings suggest the co-existence of a triple burden of malnutrition in Tanzanian children: undernutrition, overnutrition and anaemia.
- Dietary quality was largely characterised by high intakes of cereals and grains, vegetables and legumes although the study group also had high intakes of fried foods, sweets and soft drinks. This may be responsible for the rise in overweight and obesity within the region.
- Robust, nationally-representative data for this age group has previously been unavailable in Tanzania, highlighting the importance of this analysis.
Background
More than 3,000 adolescents die every day, totalling 1.2 million deaths a year, largely from preventable causes (WHO, 2017). More than two-thirds of these deaths occur in low- and middle-income countries (LMICs) in Africa and South-East Asia (WHO, 2016). In sub-Saharan Africa, where 23% of the population is between 10 and 19 years of age, over 50% of adolescents attending school present with micronutrient deficiencies, such as anaemia, primarily due to food insecurity and limited food diversity (UNICEF, 2018). This period of adolescence is marked by significant physical and cognitive growth with broad implications on health throughout the life course. In LMICs, 500 million school days are estimated to be lost due to illness each year, contributing to significant school dropout rates and hindering the development of human capital for economic development (World Bank, 2018).
Hence, there is a focus on improving adolescent nutrition and health across sub-Saharan Africa including in Tanzania (United Republic of Tanzania, 2016). However, the paucity of data affects programming and investments in adolescent nutrition, therefore threatening gains from investments in maternal and child nutrition (WHO, 2014). This article assesses the prevalence of the types of malnutrition and the association between diet quality and nutritional status, including anaemia, among school-aged children (SAC) and adolescents in Tanzania.
Methodology
A cross-sectional School Malaria and Nutrition Survey (SMNS) was conducted among SAC (5-9 years of age) and adolescents (10-19 years of age) in mainland Tanzania between August and October 2019. A total of 68,147 pupils from 661 selected public schools were interviewed using 24-hour dietary recall to understand what foods and beverages they had consumed over the previous 24 hours. Participants were asked to recall all the food and drinks consumed from the time they woke up in the morning to the time they went to sleep at night. To assess diet quality, the consumption of a variety of food groups at least once per week was assessed using the Diet Quality Score subscale1. Items included in the subscale were chosen from the study by Lazarou et al (2010) and the DONALD study (Feskanich, 2004). In addition, information on eating habits was collected as part of the dietary assessment.
Anthropometric measurements were collected using Seca weighing scales and ShorrBoard height boards. Measurements obtained (weight and height) were used to calculate z-scores which were used to classify individual children as stunted (height for age z-score (HAZ) <-2), based on the World Health Organization (WHO) reference population, or overweight if they had a body mass index (BMI)-for-age z-score (BAZ) >1, as obese with a BAZ >2, as thin with a BAZ <-2 and severely thin with a BAZ <-3.
Anaemia status was assessed in a randomly selected sub-sample of 33% of the enrolled pupils. Haemoglobin (Hb) concentration was measured using a drop of blood obtained via a finger prick and Hb concentration was assessed using a hemoglobinometer. Hb concentration was adjusted for altitude in specific localities and the severity of anaemia was defined based on WHO cut-off points (WHO 2011).2
Descriptive statistics, including percentage, mean and minimum/maximum values, were produced using STATA and presented in tables, maps and graphs. Since our endogenous variable – BMI – was a categorical variable with more than two possible categories (underweight, normal, overweight and obesity), a multinomial logistic regression was performed to assess the association between BMI and dietary quality, controlling for the following variables: sex, age and physical activity levels. To determine the association between diet quality and anaemia, a log binomial regression model with log link function was performed. A multivariable log binomial model was used to control for confounders. All analyses were two-sided and set at the 0.05 significance level.
Findings
A total of 68,147 SAC and adolescents were recruited. The majority were female (50.2%), 10-14 years of age (58.5%, mean age = 10.7 years) and from rural areas (72.4%).
Nutrition status
Table 1 describes the prevalence of stunting, underweight, thinness, overweight, obesity and anaemia among SAC and adolescents 5-19 years of age in mainland Tanzania. 25% (17,004) were stunted, 11% (7,454) were thin and 5% (3,388) were overweight or obese. 11.7% (2,792) of the pupils 5-9 years of age were underweight.
Stunting was found to be more prevalent in older children, affecting 45.8% of those 15-19 years of age. Stunting prevalence was higher among males than females (28.4% vs. 21.6%; p<0.001) and among children living in rural areas than urban areas (27.2% vs. 19.1%; p<0.001). The prevalence of underweight was significantly higher among males (12.8% vs. 10.7%; p<0.001), children from rural areas (12.6% vs. 9.7%; p<0.001) and those who tested positive for malaria when compared to those who tested negative (16.7% vs. 8.7%; p=0.000).
The prevalence of thinness (as defined by low BAZ) was higher among boys (12.9%) than girls (10.2%), among participants between 15-19 years of age (20.2%) and among participants from rural areas (12.5%) than those from urban areas (8.9%). The prevalence of overweight was higher in girls (4.5%) than boys (3.6%), in children from the lower age group (5-9 years of age) (5.2%) than from older age groups and from urban areas (6.6%) rather than rural areas (3.0%). More urban children were affected by obesity than those from rural areas (p<0.001).
Table 1: Relationships between participant characteristics and nutritional status
Note: The table is based on school children and adolescents who were assessed for anthropometric indices. Each of the indices is expressed in standard deviation units (SD) from the median of the WHO Reference 2007 for 5-19 years to monitor the growth of school-age children and adolescents.
The table is based on children with valid dates of birth (month and year) and valid measurements of both height and weight.
*Weight-for-age reference data is not available beyond age 10 because this indicator does not distinguish between height and body mass in an ageing period where many children are experiencing the pubertal growth spurt and may appear as having excess weight (by weight-for-age) when in fact they are just tall.
The assessment of diet quality showed that the majority consumed cereals and grains (69.7%), vegetables (32.2%) and legumes (29.6%) at least five times or more per week (Table 2). Whole fried food (10.3%), soft drinks (9.6%) and meat (6.4%) were consumed the least with comparatively smaller proportions of participants consuming these at least five times or more per week.
Table 2: Frequency of the consumption of various foods and food groups among school-aged children and adolescents in Tanzania
Table 3: Association between BMI-for-age and diet quality among school-aged children and adolescents in Tanzania
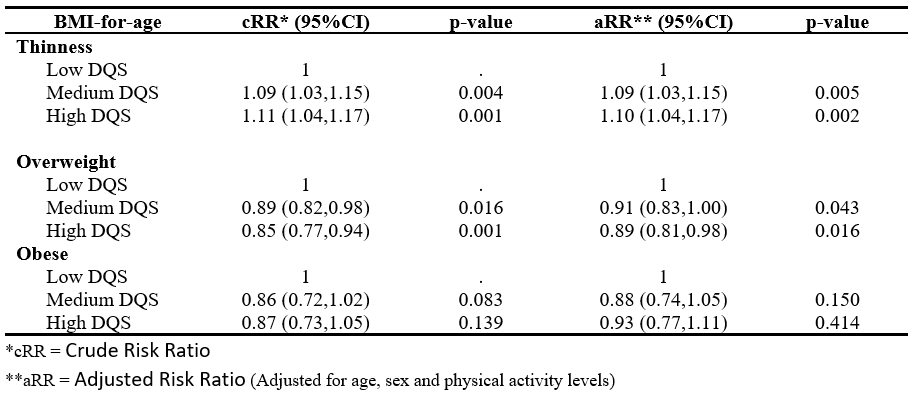
After adjusting for the effects of age, sex and level of physical activity, SAC and adolescents with medium (aRR: 0.91; p=0.043) and high diet quality (aRR: 0.89; p=0.016) had a 9% and 11% lower risk of overweight compared with those with low dietary quality respectively. Surprisingly, those with median and high dietary quality had a significantly lower risk of thinness. However, median and high dietary quality was not significantly associated with obesity (Table 3).
Anaemia
Overall, 33.9% (7,854) of SAC and adolescents who had Hb assessments were anaemic. When stratified by age, 33.1% of those 5-9 years of age, 31.5% of those 10-14 years of age and 56.6% of those 15-19 years of age had some degree of anaemia (Table 1). The prevalence of anaemia was >30% among both boys and girls as well as being higher in those from rural vs. urban areas and those with positive vs. negative malaria status.
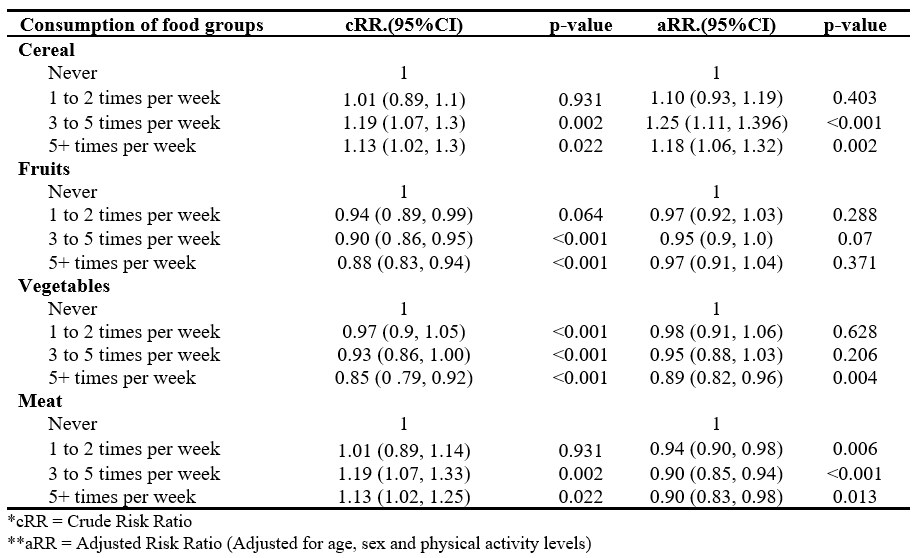
The likelihood of being anaemic was positively associated with cereal consumption and inversely associated with the consumption of vegetables (five+ times per week) and meat (at any frequency per week) (Table 4). Pupils who consumed cereals at least five or more times a week had an 18% higher risk of being anaemic compared to those who never ate cereals, while those who consumed vegetables or meat five or more times per week had a lower risk of being anaemic.
Table 4: Association between anaemia and the consumption of food groups among respondents (N= 23,167)
Geographic representation of the prevalence of malnutrition and anaemia
Maps illustrating the prevalence of stunting, anaemia and overweight according to the level of public health significance across all regions are presented in Figure 1.
Figure 1: Prevalence of stunting, anaemia and overweight among school-aged children and adolescents 5-19 years according to the level of public health significance by region
Stunting was comparatively higher in the Njombe (43.3%), Kigoma (36.2%), Kagera (34.1%) and Rukwa (33.4%) regions; the lowest prevalence was recorded in the Dar es Salaam region (14.4%). Anaemia prevalence was highest among pupils in the Pwani region (53.3%) and lowest in the Iringa region (13.4%). Overweight prevalence was highest in the Lindi region (7.2%) followed by the Mbeya and Morogoro regions (both 6.8%).
Discussion and limitations
Robust nationally-representative data for SAC and adolescents (5-19 years of age) has not been available in Tanzania which has hindered the inclusion of nutrition in national policies, strategies, guidelines and plans for this vulnerable group. The nationally-representative data presented here provides the evidence required to support efforts to improve nutrition in this demographic in Tanzania.
The findings indicate the co-existence of undernutrition, overnutrition and anaemia in SAC and adolescents. We found that girls are less likely to be stunted than boys which aligns with existing evidence from the region (Bork, 2017). Sex differences in nutritional status, particularly stunting, are poorly understood – various potential drivers exist including poorer neonatal outcomes in males (Elsmén, 2004), preferential treatment among female children in some communities (Svedberg, 1990) and higher morbidity among male children (Green, 1992). Stunting prevalence was also lowest in the younger age groups. This could be partly explained by the increase in nutritional interventions and an improvement in the nutrition status of women over recent years, corresponding with a steady decline in stunting among the younger children in Tanzania. As demonstrated previously (Nicholaus et al, 2020), rates of overweight and obesity are increasing in the country with females being more at risk than males.
Dietary quality among SAC and adolescents was largely characterised by high intakes of cereals and grains, vegetables and legumes (beans, peas and nuts). Previous research has reported increasing consumption of high-calorie foods among SAC and adolescents especially in urban areas (Ochola and Masibo, 2014). The data presented here similarly demonstrates high intakes of fried food and sweets (junk food) and soft drinks. A similar study from Kenya reported that the majority of primary school children consumed sweetened beverages and junk foods, including chips, sweets, sausages, doughnuts and chocolate, in the seven days prior to assessment (Kigaru et al, 2015). The consumption of readily available, high-energy food items is a major contributing factor to the rise in overweight and obesity as well as noncommunicable diseases in Tanzania and the region. To tackle this, there is a need to promote healthy diets in schools and improve school health and nutrition environments. Efforts should include integrating nutrition into the school curriculum, creating school gardens to promote the consumption of vegetables and fruits and increasing the uptake of other nutrition-sensitive interventions such as water, sanitation and hygiene and deworming programmes.
Our survey showed that anaemia was common among SAC and adolescents in Tanzania with disparities across age groups, sex and geographical regions. The oldest age group reported an anaemia prevalence categorised as severe according to WHO guidelines, with the younger age groups categorised as moderate. Higher anaemia prevalence was also observed among children who tested positive for malaria, suggesting that malaria is contributing to the high levels of anaemia observed. Anaemia is associated with increased absenteeism, poor educational performance and increased school dropouts among SAC (Leslie et al., 1990). Weekly micronutrient supplementation may contribute to anaemia reduction and improved health outcomes and education performance among SAC and adolescents (WHO, 2018).
It is important to note the limitations of this analysis. The SMNS is a cross-sectional survey so data cannot be used to assess causality. Dietary assessment methods did not account for seasonal variations and the list of food items included in the food frequency questionnaire was not exhaustive. As a result, it was not possible to establish consumption patterns based on a specific season or food item. The timing of the SMNS data collection varied by region therefore indicators affected by seasonality should be compared and interpreted with caution. In addition, the study used a dietary assessment tool that is not validated in developing countries.
Conclusion
The SMNS findings indicate the existence of the triple burden of malnutrition among SAC and adolescents in Tanzania, posing a growing health challenge. The identification, promotion and implementation of both nutrition-sensitive and nutrition-specific actions that simultaneously and synergistically address undernutrition, overweight/obesity (and diet-related noncommunicable diseases) and micronutrient deficiencies in line with the Tanzania National Multisectoral Nutrition Action Plan provides an important opportunity to improve the nutrition and health status among this demographic. We recommend a joint multi-sector response towards the sustainable scale-up of a comprehensive nutrition programme with an intensified focus on making healthy diets accessible and affordable. We also recommend innovative approaches to address the built environment in and around schools and social and behaviour change communication approaches tailored to reach most children and adolescents through schools, as well as other community-based platforms.
For more information, please contact Sauli Epimack at sepimack@gmail.com.
1This subscale measures dietary quality or the frequency of the consumption of 11 types of foods and one cooking method. A four-point scale is used based on recommended nutritional items and frequencies. Response choices are never, once per week, two to four times per week and five or more times per week. Responses are weighted to reflect healthy or unhealthy frequencies with the potential score ranging between zero and 34. Higher scores indicate healthier dietary practices.
2Adolescents 15-19 years of age: any anaemia (girls: <12.0 g/dl, boys: <13.0 g/dl), mild anaemia (girls: <11.0–11.9 g/dl, boys: <11.0–12.9 g/dl), moderate anaemia (8.0–10.9 g/dl) and severe anaemia (<8.0 g/dl). SAC 5-9 years of age: any anaemia (<11.0 g/dl), mild anaemia (11.0–11.4 g/dl), moderate anaemia (8.0–10.9 g/dl) and severe anaemia (<8.0 g/dl).
References
Bailey, RL, West Jr, KP and Black, RE (2015) The epidemiology of global micronutrient deficiencies. Annals of Nutrition and Metabolism, 66(Suppl. 2), 22-33.
Bhutta, ZA, Das, JK, Rizvi, A, Gaffey, MF et al (2013) Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? The Lancet, 382(9890), 452-477.
Bork, KA, Diallo, A (2017) Boys Are More Stunted than Girls from Early Infancy to 3 Years of Age in Rural Senegal, The Journal of Nutrition, Volume 147, Issue 5, May 2017, Pages 940–947
Elsmén, I, Pupp, HI, Hellström-Westas, L (2004) Preterm male infants need more initial respiratory and circulatory support than female infants. Acta Paediatr., 93: 529-533. 10.1080/08035250410024998.
Feskanich, D, Rockett, H and Colditz, G (2004) Modifying the healthy eating Index to assess diet quality in children and adolescents. Journal of the American Dietary Association, 104, 1375-1383
Green, MS (1992) The male predominance in the incidence of infectious diseases in children: a postulated explanation for disparities in the literature. Int J Epidemiol. 21: 381-389. 10.1093/ije/21.2.381.
Kigaru, DMD, Loechl, C, Moleah, T, Macharia-Mutie, CW and Ndungu, ZW (2015) Nutrition knowledge, attitude and practices among urban primary school children in Nairobi City, Kenya: a KAP study. BMC Nutr 1, 44. https://doi.org/10.1186/s40795-015-0040-8
Lazarou, C and Kouta, C (2010) The role of nurses in the prevention and management of obesity. British Journal of Nursing, 19(10), 641-647.
Leslie, J and Jamison, DT (1990) Health and nutrition considerations in education planning. 1. Educational consequences of health problems among school-age children. Food and nutrition bulletin, 12(3), 1-13
Nicholaus, C, Martin, HD, Kassim, N, Matemu, AO and Kimiywe, J (2020) Dietary practices, nutrient adequacy, and nutrition status among adolescents in boarding high schools in the Kilimanjaro region, Tanzania. Journal of Nutrition and Metabolism. https://doi.org/10.1155/2020/3592813
Ochola, S and Masibo, PK (2014) Dietary intake of schoolchildren and adolescents in developing countries. Annals of Nutrition and Metabolism. 64(Suppl. 2): p. 24-40.
Svedberg, P (1990) Undernutrition in sub-Saharan Africa: is there a gender bias. J Dev Stud., 26: 469-486.
Temple NJ et al. (2006) Food items consumed by students attending schools in different socioeconomic areas in Cape Town, South Africa. Nutrition, 2006. 22(3): p. 252-258.
UNICEF (2012) Progress for Children. A report card on adolescents. Number 10, April 2012. https://www.unicef.org/media/86401/file/Progress_for_Children_-_No._10_EN_04272012.pdf. Accessed on 20th July 2021.
UNICEF (2018) Adolescent Health, The Missing Population in Universal Health Coverage
United Republic of Tanzania (2016) National Multisectoral Nutrition Action Plan (NMNAP) for the period July 2016 – June 2021.
WHO (2014) Health for the world's adolescents: a second chance in the second decade: summary. World Health Organization. https://apps.who.int/iris/handle/10665/112750
WHO (2016) Global health estimates 2015: deaths by cause, age, sex, by country and by region, 2000–2015. World Health Organization: Geneva (http://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html).
WHO (2017) Global Accelerated Action for the Health of Adolescents (AA-HA!): guidance to support country implementation. Summary. Geneva: World Health Organization (WHO/FWC/MCA/17.05). Licence: CC BY-NC-SA 3.0 IGO.
WHO (2018) Weekly iron and folic acid supplementation as an anaemia-prevention strategy in women and adolescent girls: lessons learnt from implementation of programmes among non-pregnant women of reproductive age. Available at: https://apps.who.int/iris/handle/10665/274581
WHO (2018) Guideline: implementing effective actions for improving adolescent nutrition. Available at: https://apps.who.int/iris/handle/10665/260297
World Bank (2018) Child and Adolescent Health and Development; Optimizing Education Outcomes: High-Return Investments in School Health for Increased Participation and Learning. The World Bank Group.