
Understanding sex differences in childhood malnutrition
This is a summary of the following paper: Thurstans S, Opondo C, Seal A, Wells J, Khara T, Dolan C et al (2021) Understanding sex differences in childhood undernutrition: A narrative review. Nutrients, 14, 5, 948. https://www.mdpi.com/2072-6643/14/5/948
Susan Thurstans is a PhD candidate at the London School of Hygiene and Tropical Medicine as well as a consultant to ENN on the Wasting and Stunting project.
Background
A recent systematic review and meta-analysis on sex differences in malnutrition in children under five years of age (Thurstans et al, 2020) found that, in most settings, boys were more likely to be wasted, stunted and underweight than girls. This research summary aims to understand the possible origins, pathways and consequences of these sex differences which may have implications for policy and practice.
Demographic variations in malnutrition by sex
A recent analysis of Demographic and Health Survey (DHS) data from Africa found that sex differences are more pronounced in children with concurrent wasting and stunting compared with those with only one deficit (Garenne et al, 2021). Sex differences may also be more pronounced among lower socio-economic groups and at higher levels of food insecurity. For example, DHS data from 16 countries in sub-Saharan Africa (Wamani et al, 2007) showed that sex differences in stunting were more pronounced as socio-economic strata declined. A separate analysis in this review found the difference in prevalence between boys and girls was increased with decreasing wealth so that there was a trend towards less pronounced sex differences in wealthier countries. While the pattern was not uniform, and the comparison would benefit from more in-depth analysis, it suggests that addressing socio-economic inequalities may contribute to reducing sex differences in malnutrition (Figure 1).
Figure 1: Prevalence of stunting only in boys and girls by level of food insecurity1
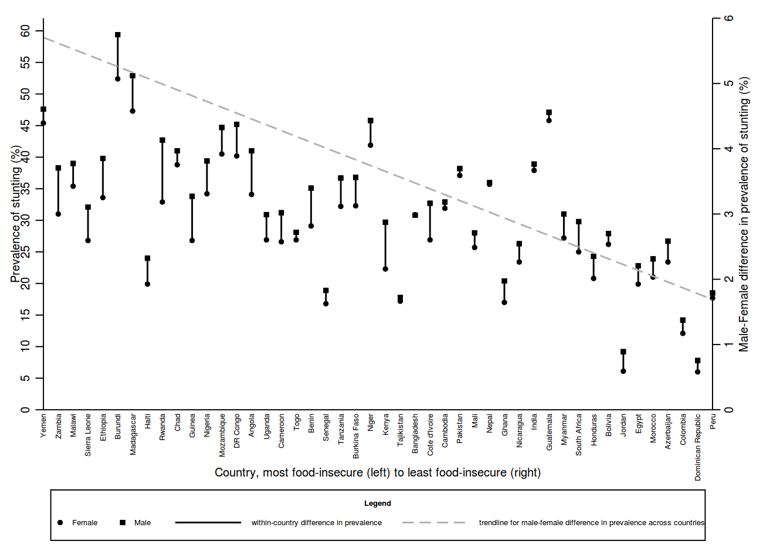
Data sources: Country food security scores from the Global Food Security Index found at: https://foodsecurityindex.eiu.com/Index. Stunting prevalence data from the DHS StatCompiler found at: https://www.statcompiler.com/en/
Potential explanatory factors for sex differences
Maternal and newborn factors
The observed sex differences appear to originate, at least in part, in utero. Male foetuses are known to be at an increased risk of poor outcomes compared to female foetuses. It is estimated that a newborn female is physiologically similar to a male at four to six weeks of age (Kraemer et al, 2000), suggesting that females are more developed at birth and potentially better able to withstand adverse conditions.
Male foetuses are, on average, larger than female foetuses between the eighth and twelfth week of gestation, suggesting that a genetic mechanism may underlie sex differences in foetal size. It is thought that male foetuses grow faster in the womb from the early stages of gestation and that males’ placentas may be more ‘efficient’ than those of females. Male placentas are smaller – by ratio to birthweight – to accommodate a larger foetus in the womb and so male placentas potentially have reduced reserve capacity (Eriksson et al, 2010). This accelerated growth may be beneficial in the presence of an abundant food supply but this makes males vulnerable to food shortages.
Similarly, evidence suggests that male foetuses are more responsive to a mother’s gestational diet than female foetuses for whom development seems more closely associated with the mother’s longer-term nutritional status. Findings from a study conducted in Nepal showed that in a population with high levels of maternal undernutrition, mothers of sons did not demonstrate greater nutrition reserves to meet the extra absolute energy costs of nourishing males when compared to females (Saville et al, 2021). Thus, boys demonstrated higher rates of stunting and lower head girths during early life.
Endocrine/immune factors
Overall morbidity and mortality rates are higher in males compared to females throughout life. One explanation for this is a stronger immune response and capacity to produce antibodies in girls. Hormonal systems also differ between boys and girls and the interaction between sex hormones and environmental factors has consequences for energy consumption, nutritional requirements and vulnerability to infectious and non-communicable diseases.
Infant and young child feeding
Methods of infant feeding have consequences for growth and development with some evidence to suggest that the quality and quantity of milk produced by breastfeeding mothers, or taken in by infants, can vary by sex. However, the evidence is limited and sample sizes are often small. In addition, a number of studies have shown that boys often receive complementary food earlier than girls, either because boys are perceived as being hungrier or because breastmilk is viewed as inferior to complementary foods and boys may be prioritised for the ‘superior’ option.
Gender perceptions
In addition to feeding and care practices, the social and economic circumstances in which families live and in which children are raised influence health and nutrition outcomes through variations in how children are fed, what services they can access and the wider health and disease environment to which they are exposed. The roles that boys and girls assume within a community, and the values attached to them, might affect both the nutritional inputs available to them and their exposure to disease and infection. For example, gender roles can influence where boys and girls spend their time and, in turn, the environment to which they are exposed and their access to food.
Indicators of malnutrition
How malnutrition is assessed and defined has potential consequences for understanding how sex differences play out. The 2006 World Health Organization growth standards use sex-specific growth references. However, what is not certain is whether the sex differences observed in this original reference population are representative of sex differences in all other populations, particularly those living in situations of deprivation. In other words, it is unclear if a specific z-score (<−3, for example) in a girl or boy of the same age corresponds to the same physiological impact in both sexes and how the distribution of fat and fat-free mass affects this. In contrast, the use of mid-upper arm circumference (MUAC) is based on a single cut-off point for girls and boys. The fact that boys are bigger in absolute terms, and have higher energy needs to grow along given centile lines, could mean that the same absolute supply of energy would only meet the requirements of a boy with a thinner arm compared to a girl. Thus, it has been suggested that using a single cut-off point for MUAC may result in the overestimation of wasting in girls and the underestimation of wasting in boys (Tadesse et al, 2017).
Possible implications of sex differences for addressing malnutrition
Although the evidence clearly shows a higher risk of wasting, stunting and underweight in boys compared with girls, more detailed analysis is needed to better understand the implications for health and nutrition. In a study of children in Senegal with concurrent wasting and stunting, sex differences in mortality were not significant after controlling for stunting and wasting (Garenne et al, 2019).
In relation to treatment, evidence is limited but might indicate longer recovery times in boys. Data from a malnutrition treatment programme in Uganda showed that girls had an increased probability of recovery than boys although the difference was not significant (Odei Obeng-Amoako et al, 2020).
Conclusion
This review highlights the complexity and, at times, conflicting nature of the evidence on the determinants of sex differences on malnutrition. Further investigation into the pathways and drivers of these differences is needed to inform appropriate programming and policy. While these findings should not undermine the efforts to address other areas of gender inequity, programme staff and policymakers should be aware of boys’ vulnerability in relation to infant and child survival, nutrition and development thus facilitating the accurate interpretation of data to ensure that all vulnerable children are identified and targeted in programmes.
References
Eriksson J, Kajantie E, Osmond C, Thornburg K and Barker D (2010) Boys live dangerously in the womb. American Journal of Human Biology, 22, 3, 330-335.
Garenne M, Myatt M, Khara T, Dolan C and Briend A (2019) Concurrent wasting and stunting among under-five children in Niakhar, Senegal. Maternal & Child Nutrition, 15, 2, e12736.
Garenne M, Thurstans S, Briend A, Dolan C, Khara T, Myatt M et al (2021) Changing sex differences in undernutrition of African children: findings from Demographic and Health Surveys. Journal of Biosocial Science, 1-11.
Kraemer S (2000) The fragile male. British Medical Journal 321, 1609-12.
Odei Obeng-Amoako G, Wamani H, Conkle J, Aryeetey R, Nangendo J, Mupere E et al (2020) Concurrently wasted and stunted 6-59 months children admitted to the outpatient therapeutic feeding programme in Karamoja, Uganda: Prevalence, characteristics, treatment outcomes and response. PLoS ONE, 15, 3, e0230480.
Saville NM, Harris-Fry H, Marphatia A, Reid A, Cortina-Borja M, Manandhar DS et al (2021) Differences in maternal and early child nutritional status by offspring sex in lowland Nepal. American Journal of Human Biology, e23637.
Tadesse AW, Tadesse E, Berhane Y, Ekström E (2017) Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia. Nutrients, 9(3): 267. https://doi.org/10.3390/nu9030267.
1 Data sources: country food security scores from the Global Food Security Index available at: https://foodsecurityindex.eiu.com/Index; stunting prevalence data from the Demographic and Health Survey (DHS) StatCompiler, available at: https://www.statcompiler.com/en/