By Dr Malam Kanta Issa
View this article as a pdf
Lisez cet article en français ici
Dr Malam Kanta Issa has worked as the Head of Mission for ALIMA Mali since 2015. After obtaining his doctorate in medicine he worked for MSF in Niger for several years before joining ALIMA in 2013, obtaining an MSc in Public Health the same year.
Location: Mali
What we know: Well-trained health professionals are needed to ensure quality inpatient treatment of children with severe acute malnutrition (SAM).
What this article adds: In Mali state capacity to provide quality inpatient treatment for SAM with complications is limited by damage to health infrastructures, staff shortages and high staff turnover, and lack of sustained, high-quality pre-service and in-service training for health professionals. A Units of Recovery and Intensive Nutrition Education (URENI) teaching hospital was established in 2015 by AMCP/ALIMA with UNICEF and Ministry of Health support to deliver a three-week, intensive, hands-on training on complicated SAM treatment for selected staff. Regional nutrition focal points (NFPs) from five districts (who monitor the integrated management of acute malnutrition) received refresher training. From 2015 to 2017, 262 Malian health professionals were trained from 41 health facilities through 22 training courses. All trainees passed the training (50% or above in final evaluation) and returned to their URENI with agreed action plans to implement changes. Plans are to train health professionals from conflict-affected northern regions not yet covered, pending funding.
Context
Mali currently has the sixth-highest infant mortality rate in the world (UNICEF, 2016) and ranks 175 out of 190 in the Human Development Index (UNDP, 2016). An annual population growth rate of 3.6% and a total fertility rate of seven children per woman contributes to constrained household resources, negatively impacting child health and nutrition. Acute malnutrition is a serious public health problem, exacerbated by the 2012 political and security crisis. Prevalence of severe acute malnutrition (SAM) is 2.1% (caseload of 142,527 children) and prevalence of global acute malnutrition (GAM) is 10.7% (622,368 children) (INSTAT, 2016). Nearly 20% of SAM cases, or more than 28,000 children, are likely to have medical complications that require inpatient treatment. Without such treatment there is an imminent risk of mortality.
Treatment of SAM in Mali
Mali has 65 Units of Recovery and Intensive Nutrition Education (URENI), where inpatient care for SAM children with complications is provided. URENI are usually integrated into the paediatric service within the reference health centre (CSREF), a secondary healthcare facility at the district level
1. However, the ongoing crisis in northern Mali has severely hampered the state’s capacity to provide quality care for children with SAM due to damage of health infrastructure and equipment, looting of medical supplies and the massive outflow of qualified medical staff. Public use of health facilities is constrained by cost, access and perceptions of the quality of care provided. Major shortages in human resources in health facilities are a critical concern (Human Resources Statistical Yearbook of Health, Social Development and the Advancement of Women, 2016). In 2016, the ratio of health professionals (doctors, midwives and nurses) in the country was 5.2 per 10,000 inhabitants. This figure, which includes state professionals and private, part state-owned and religious organisations, is well below the WHO standard (23 per 10,000). This problem is particularly marked in rural areas: the ratio falls to 3.9 health professionals per 10,000 inhabitants when the capital, Bamako District, is excluded. Poor availability of qualified health staff in remote areas is further complicated by the security situation in central and northern regions of the country.
ALIMA in Mali
The Alliance for International Medical Action (ALIMA) is a medical humanitarian organisation created in 2009. It brings together the medical expertise of international humanitarian workers, national medical NGOs and global research institutes to provide quality medical assistance to the most vulnerable and conduct research projects to advance humanitarian medicine. ALIMA operates in the Sahel (Niger, Mali, Burkina Faso and Chad), the Democratic Republic of the Congo, the Central African Republic, Guinea, Cameroon and northern Nigeria. Its regional office is in Senegal.
ALIMA operates in Mali with its national partner, the Medical Alliance Against Malaria (AMCP), founded in 2010. In the Koulikoro region, AMCP/ALIMA have been present since 2011 in the districts of Fana, Dioïla, Kolokani, Ouéléssébougou, Kangaba and Koulikoro, supporting nutrition and health treatment in government health structures. The project supports 111 community health centres (CSCOMs), which operate at health area level, and six district CSREFs in caring for children under five years old with SAM and malaria. AMCP/ALIMA has also been present in the Timbuktu region since March 2012 to meet the health needs created by the crisis in northern Mali and has supported the health structures in the districts of Diré and Goundam since 2012. At the end of 2016, AMCP /ALIMA supported all health structures in the district of Diré (one CSREF and 18 CSCOMs) and two thirds of the functional health structures in the district of Goundam (one CSREF and 17 CSCOMs). In Diré and Goundam the project focuses on access to free, high-quality primary and secondary healthcare, including support for paediatrics, maternity, internal medicine and surgery.
Gaps in health staff competencies
Although treatment of malnutrition should be considered a public health priority, Malian health professionals lack competence in this area. Modules dedicated to the treatment of malnutrition and the management of SAM with complications rarely feature in standard training curricula for Malian doctors. In addition, the academic curriculum in Mali lacks practical training in important aspects specific to the nutritional and medical treatment of complicated SAM, such as diagnosis, additional examinations indicated, medical supervision, delivery of emergency treatment, management of complications (such as rehydration, transfusions and oxygen therapy) and compliance with hospital hygiene standards. As a result, there is great potential for medical errors, leading to increased mortality. Beyond the gaps in the theoretical and practical knowledge of health staff, ongoing training in treatment protocols related to malnutrition and associated pathologies often suffers from a lack of rigour and continuity. These issues are compounded by high staff turnover in marginalised areas that generates substantial recurrent training needs for those treating particularly marginalised and vulnerable populations.
Short-term capacity development
Non-governmental organisations (NGOs) support URENI and CSREF capacity development through annual updates on best-practice medical and nutritional care for medical staff. However, these training courses are short-term interventions carried out by non-permanent organisations. In addition, in 2017 there was a sharp reduction in support from financial partners for nutrition activities in the country, which led to decreased NGO support for nutrition activities to health districts. State funds have not yet been provided to compensate for this change and are likely to remain low and insufficient. The humanitarian aid appeal for Mali in 2017 includes a request for US$58 million for nutrition interventions; yet to date only 11% of these resources have been mobilised (OCHA, 2017). This lack of funds, coupled with inadequate human resources, increases the risk of deterioration in the quality of care and child mortality.
Building competencies: URENI teaching hospital
In response to these needs, the URENI teaching hospital was set up by AMCP/ALIMA in Dioila during the second half of 2015 in partnership with UNICEF and the Nutrition Division (DN) of the Ministry of Health (MoH). It is integrated within the CSREF in Dioila. Its objective is to strengthen the skills and knowledge required for the inpatient care of severely malnourished children. The project focuses on addressing obstacles in providing high quality of care in the URENIs, as observed by AMCP/ALIMA since 2011. A three-week training programme was established at the URENI teaching hospital based on educational modules validated by the DN of the MoH and UNICEF and is supervised by experienced medical staff.

Hands-on training
The training is based on the ‘learning-by-doing’ method, which allows both reflective observation and active engagement of trainees, who learn through practice. Skills and knowledge are acquired by trainees who accompany the nurses and doctors of Dioila CSREF in the nutritional and medical care of SAM children with complications. Trainee doctors conduct joint visits to the URENI and paediatric ward with the responsible physician. Trainee nurses work in pairs with URENI nurses; the ALIMA deputy supervisor nurse guides the trainees in acute and transition phases while the ALIMA senior nurse accompanies them in intensive care, to provide close educational support.
Daily medical meetings are held to discuss complicated cases in depth. Weekly medical meetings are also held for the Dioila medical team and trainees to review complicated clinical cases, deaths and causes of mortality. In addition, thematic presentations are made twice weekly; topics are selected according to the needs identified by the pedagogical supervision team and have included SAM monitoring, SAM rehydration, calculation of therapeutic food doses and administration of drugs, procedures in the case of exposure to blood, transfusion prescription and monitoring, emergency treatment of shock, hospital hygiene, and preparation of therapeutic milk and diet for SAM children.
Trainees spend time at the pharmacy to understand pharmaceutical management principles (storage organisation, drug conservation and tools for pharmacy management such as stock sheets, application of FEFO (first-expired, first-out) rules on expiry dates and the principles of cold chain management). In addition, trainees spend time with the logistician and hygienists on waste management and sanitation in Dioila CSREF. This covers subjects such as correct sorting and incineration of waste and preparation of chlorine solutions for decontamination of different tools/equipment. The doctor in charge of Dioila URENI tutors trainees on human resources (HR) management, pharmacy management (elaboration of nutritional and medical orders and the importance of carrying out regular inventory and follow-up of drug consumption) and medical data analysis.
Trainee evaluation
Trainees’ knowledge and skills/competencies are evaluated at three stages: the beginning of training (to measure initial knowledge and skills), mid-term (to measure knowledge and skills gaps to adapt the training to meet identified needs) and at the end (to measure acquired knowledge and skills).
Theoretical knowledge is evaluated through a written test that presents a series of yes/no questions and examination of practical cases (such as admission and discharge criteria, complications associated with SAM, detection of nutritional oedema, administration of therapeutic milk, treatment of dehydration and surveillance of SAM children). Practical skills are evaluated by the supervising team through daily observations of clinical practice.
Different practical and theoretical evaluations are used for trainee doctors and trainee nurses via an evaluation grid of quality standards in each phase of treatment. For example, in the acute phase trainee doctors must master around 40 technical competencies, grouped into six categories: diagnosis and treatment of SAM with complications, treatment of breast-fed infants under six months old or infants weighing less than 3kg, medical activities (for example, use of a urinary catheter, use of an intravenous needle and performing a lumbar puncture), record-keeping, quality of medical prescriptions and data analysis.
Evaluation standards are based on the national protocol for integrated management of acute malnutrition (PECIMA) and trainees must obtain a score of at least 50%. If a trainee does not meet the required standard by the end of the training, they are referred to UNICEF to liaise with the CSREF of origin to arrange a plan for specific support. As trainees are evaluated three times and closely supervised throughout the internship, to date none have obtained a score below 50%.
Trainees also formulate their own expectations regarding the internship and themes they would like to cover during their training and identify five objectives they would like to achieve by the end of the internship. The trainees are responsible for implementing the protocols and care practices learned during the training in Dioila within their local CSREF. At the end of the programme, trainees draw up an action plan for the management of SAM cases in their local CSREF based on their knowledge of materials and human resources available in their CSREF of origin. This document helps guide the trainees once they return to their own URENI and contributes to the spread of good organisational and management practices in healthcare facilities.
Refresher training of nutrition focal points (NFPs)
Regional nutrition focal points (NFPs) oversee monitoring the integrated management of acute malnutrition (PECIMA) at the regional level and have an important role in the supervision and evaluation of the URENIs and their staff. They are employed by the DN, which is part of the National Office for Health, under the responsibility of the MoH. One NFP per sanitary district has been deployed in accordance with the PECIMA. Monitoring and evaluation tools used by NFPs include a performance evaluation grid, designed by the MoH to monitor and evaluate the URENIs. Data provided by NFPs are reviewed by each Regional Health Director and then sent to the national-level DN. The NFPs in Koulikoro, Bamako, Mopti, Ségou and Kayes have benefited from a refresher course at the URENI school, helping to improve their techniques for monitoring and evaluating all URENIs. NFP training focused on frequency of supervision, use of existing monitoring tools, editing supervision reports and data collection. The follow-up plans produced by trainee doctors and nurses in their region were shared with the relevant NFP.
Outcomes of the URENI teaching hospital training
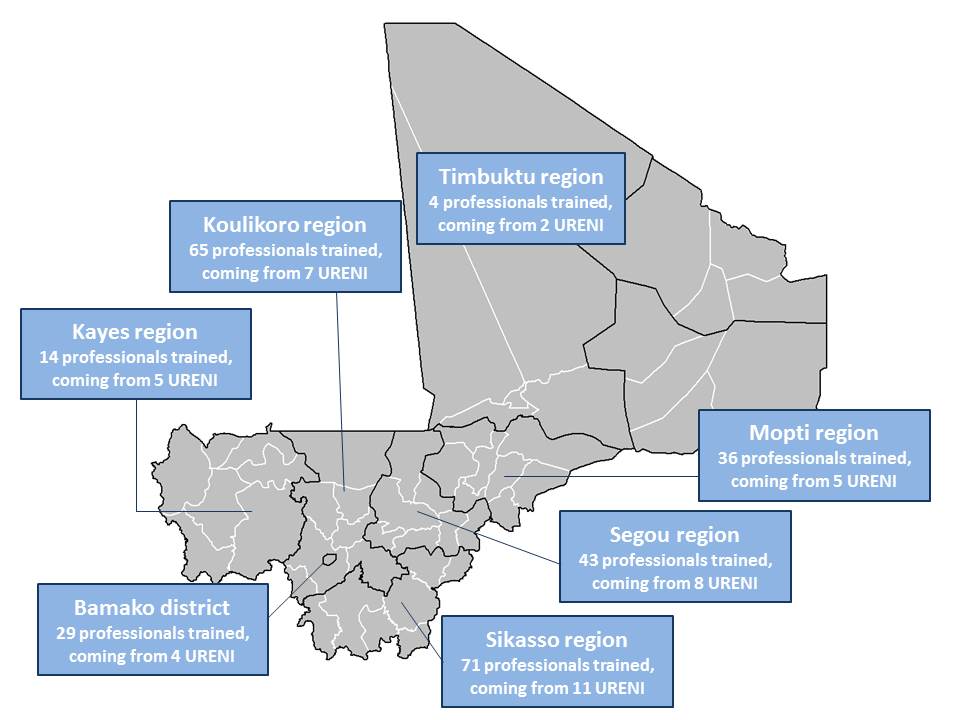
Between August 2015 and April 2017, the project trained a total of 262 Malian health workers, including 67 doctors from 41 health facilities. Figure 1 displays the regions from which health workers originated. Trainees were identified by UNICEF in collaboration with the CSREF of origin and ALIMA. Priority was given to CSREFs that were not supported by an NGO for nutritional activities. The trainees were evaluated on 40 medical and nursing procedures. The 22 training courses delivered had a 100% success rate (all trainees scored above 50% on final examination). At the end of the practical training, all participants could apply national and international care standards for SAM with complications.
Figure 1: Map of URENI teaching hospital trainees regions of origin
Staff at Dioila CSREF had no objections to integrating the training into their regular work and did not receive extra payment; the added value was clear for all involved. While difficult to quantify the extra time required by regular employees, extra staff were recruited by ALIMA at the outset to strengthen CSREF capacity. This was a necessary part of the improvement in inpatient care at the URENI and to ensure trainees were properly managed. In total, 11 ALIMA/AMCP staff were recruited and funding was provided to support 42 workers at the URENI, including six doctors and 20 nurses.
While releasing staff for training was not an issue for doctors and nurses, it was challenging for NFPs who struggled to attend for three whole weeks, the initial length of their supervision training. Training was reduced to two weeks as a result. Interestingly, trainees fed back that even three weeks was too short. There are no practical training programmes for health workers at a lower level; however they can benefit from theoretical trainings provided by the MoH.
There are some significant barriers to full implementation of good practices and standards acquired during the training. The most common ones are the lack of suitable premises and medical equipment (specific tools such as otoscopes, glucometers and saturometers) and insufficient human resources. Addressing these requires financial and material support from the state; this in turn requires strong advocacy and the involvement of every stakeholder, from NFPs and district head doctors to laboratory and pharmacy managers.
Discussion and conclusions
The URENI training hospital brings together emergency medicine and development, since it both supports children with a high risk of mortality and develops the skills of Malian health workers, thus developing resilience in the health system. The main outcomes of the programme have been to provide a response to structural training needs in the face of the endemic nature of SAM in Mali; to prepare for future nutrition and health crises; and to strengthen capacity to respond to crises in the most challenging regions, particularly in northern Mali, where there are urgent needs. ALIMA has received very positive feedback on the training initiative and no significant changes to the approach are planned.
In the future, the URENI training hospital plans to train health professionals from conflict-affected northern regions (Gao, Timbuktu, Taoudenit, Menaka and Kidal) and central regions (Segou and Mopti) in CSREFs that do not currently receive support from an NGO in the management of malnutrition. The hospital plans to train eight health professionals per CSREF in these areas who have not yet benefited from the internship. Several grant applications have been submitted to donors to secure finance for the URENI training hospital.
With regard to the long-term goal of improving the treatment of children affected by SAM, we believe it is necessary to implement some complementary programmes, such as training in management of less complicated cases of malnutrition and training on early case identification. There is a real need for improvement of SAM treatment, but we also need to consider ways to reduce the number of children with complicated cases who require hospitalisation.
For more information, contact: Dr Malam Kanta Issa mali@alima-ngo.org
Endnotes
1There are four health divisions in Mali: state, region, district and health
References
2016 Human Resources Statistical Yearbook of Health, Social Development and the Advancement of Women (February 2017)
INSTAT 2016. National Statistics Institute of Mali (INSTAT). Nutrition and retrospective mortality SMART survey, Mali, July 2016.
OCHA 2017. United Nations Office for the Coordination of Humanitarian Affairs (OCHA) Financial tracking service (FTS) 2017. https://fts.unocha.org/
UNDP 2016. United Nations Development Programme. Human Development Report – 2016 HDR Report. http://hdr.undp.org/en/countries/profiles/MLI
UNICEF 2016. UNICEF Data. Monitoring the Situation of Children and Women: Under-five Mortality. October 2016 (updated). https://data.unicef.org/topic/child-survival/under-five-mortality/

