
From cluster to Nutrition Sector coordination: Government leadership in coordination for effective nutrition emergency response in Borno State, Nigeria
By Maureen L Gallagher, Kirathi Reuel Mungai, Ladi Linda Ezike and Dr Helni Mshelia
Maureen L. Gallagher is a nutrition specialist with UNICEF’s Emergency Response Team based in UNICEF HQ, New York. She is a public health specialist with over 15 years’ experience in nutrition programming. She has been deployed to support the emergency response in Nigeria, Yemen and Democratic Republic of Congo.
Kirathi Reuel Mungai is a nutrition specialist currently working with UNICEF as a Nutrition Sector coordinator in Nigeria, based in Borno. He has worked as a public health nutritionist for the last 11 years in Kenya, South Sudan and Nigeria for UNICEF, Action Against Hunger, Concern Worldwide, World Food Programme and the Government of Kenya. He has also worked as the Nutrition Cluster Coordinator in South Sudan.
Ladi Linda Ezike is the State Nutrition Officer for the Government of Borno State Nigeria, where she is the focal point for coordination and collaboration with all nutrition partners and oversees nutrition activities. She has worked with the Borno State Ministry of Health for over 30 years, including the last five years of the Boko Haram emergencies.
Dr Helni Mshelia is a public health specialist and medical doctor. She is presently the Director of Primary Health Care for the Borno State Primary Health Care Development Agency (SPHCDA), where nutrition is one of the key areas of her responsibility. She has coordinated all nutrition interventions in the state since the start of the Boko Haram emergency and is pioneer chair of the Borno State Nutrition Sector coordination group.
The authors would like to thank the Government of Nigeria at federal, state and local government levels as well as partners for their collaboration in fighting undernutrition in Nigeria. The authors would also like to thank Dominic Stolarow and Simeon Nanama for their valuable contributions to this article and Sultan Ahmed for the infographics used here.
The findings, interpretations and conclusions in this article are those of the authors. They do not necessarily represent the views of UNICEF, its executive directors or the countries that they represent and should not be attributed to them.
Location: North-eastern Nigeria (NE Nigeria)
What we know: NE Nigeria is currently experiencing mass population displacements due to internal conflict, aggravating a chronic serious problem of child undernutrition.
What this article adds: Borno State has been most affected by the current crisis (1.4 million people displaced), requiring a coordinated, multi-sector emergency nutrition response. Emergency nutrition coordination has built on existing development coordination mechanisms, located within the health sector with UNICEF support to government. The cluster system was not activated. The health system is devolved and leadership is strong at state level, with necessary links to federal arrangements. Coordination has been established at sub-state level to meet heightened coordination needs. Government leadership has facilitated considerable collaboration, including geographic mapping at ward level to identify gaps; development of a response plan aligned with national nutrition plans and policies; an integrated nutrition services minimum package and sector information database; a harmonised approach to human resources; and establishment of a nutrition surveillance system. Tripartite partnerships between government, non-government organisations and UNICEF aim for service quality. Government-led coordination has been enabled by strong high-level leadership, political will for an effective response and adequately resourced coordination capacity.
Prior to the Boko Haram conflict, Adamawa, Borno and Yobe states in North-eastern Nigeria (NE Nigeria) ranked below southern states on key socioeconomic indicators, with a poverty rate among the highest in the country at 69 per cent (World Bank Group, 2016). The prevalence of stunting among children under five years old of 47 per cent in Adamawa and Borno and 65 per cent in Yobe was above the national average of 36 per cent (NBS/UNICEF, 2010). Prevalence of wasting varied between the three states and was highest in Yobe. Poor feeding practices also prevailed, with only 12 per cent and 2.7 per cent of mothers in Borno and Yobe States respectively practicing exclusive breastfeeding (NBS/UNICEF, 2012). This already serious undernutrition situation in NE Nigeria was further aggravated with the escalation of insecurity caused by Boko Haram in 2013.
Mass displacement continues to sustain chronic underdevelopment in Adamawa, Borno and Yobe States. According to the IOM (2017), the majority of internally displaced persons (IDPs) remain in Borno (1,439,940), followed by Adamawa (140,875), and Yobe (107,201), with 96 per cent of IDPs reporting displacement due to the ongoing Boko Haram conflict. The majority of the 1.7 million IDPs across the north-east states are among the most vulnerable groups: a quarter of the IDPs are children under five years old and over half (54 per cent) of the overall population are female.
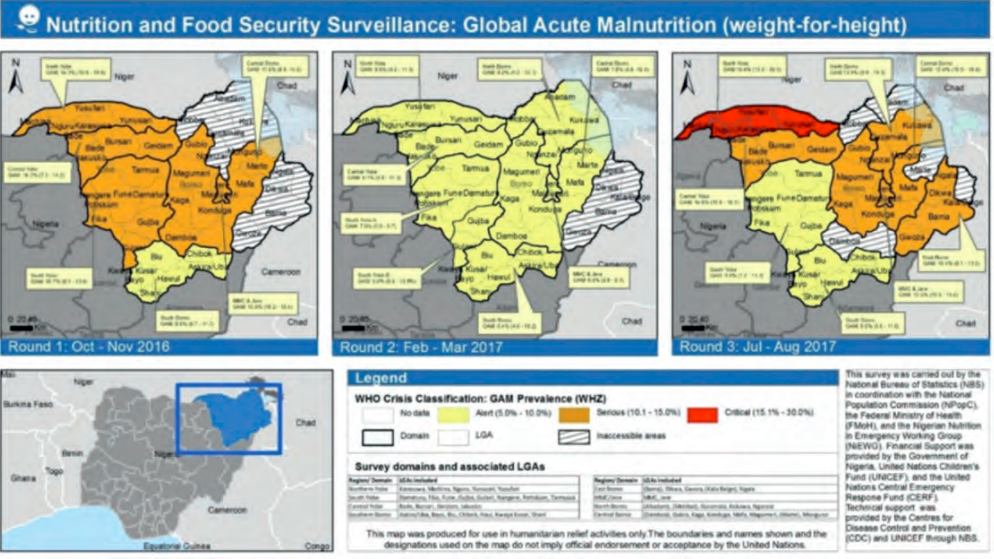
SMART nutrition assessments conducted in August 2017 indicated pockets of high malnutrition among children aged 6-59 months, with levels above the global acute malnutrition (GAM) emergency threshold rate of 15 per cent in the local government areas (LGAs) Jakusko and Northern Yobe (Karasuwa, Machina, Nguru, Yunusari, Yusufari LGAs). Serious nutrition situations (GAM between 10 and 14 per cent) were reported in Northern Borno (Abadam, Mobbar, Guzamala, Kukawa, Nganzai LGAs) and central Borno (Damboa, Gubio, Kaga, Konduga, Mafa, Magumeri, Marte, Monguno LGAs). Results are presented in Figure 1 for the three rounds of data collection completed.
Figure 1: Nutrion survey results round 3, August 2017
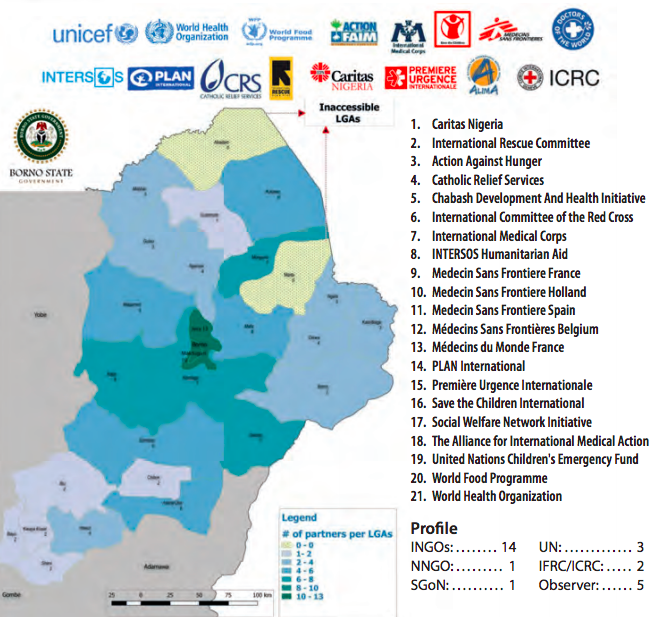
Borno has been the State most affected by the insurgency to date in terms of number of displaced people hosted and security incidents. To flee risks and violence, many households moved to new locations, resulting in over 1.4 million displaced people arriving in the main towns of LGAs and especially in the capital, Maiduguri Municipal Council (MMC), and neighbouring Jere LGAs, which host 80 per cent of all IDPs. MMC and Jere were the site of the first displacements, followed by the main towns of other LGAs when it became safe for people to move there. There has been a continued need for well coordinated, multi-sector (nutrition, health, water and sanitation and food security) scale-up of the humanitarian response across the State. Starting in 2013, as the insecurity escalated and needs increased, the number of partners supporting nutrition interventions increased from two to 18 (see figure 2 for nutrition partner presence in Borno State in 2017). The increased need for partner coordination in Borno set the stage for exploration of an improved and more sustainable mechanism for nutrition emergency response coordination.
Figure 2: Nutrition partner presence, Borno State, 2017
 History and evolution of the Nutrition Sector coordination structure
History and evolution of the Nutrition Sector coordination structure
Nigeria is a federal country, with devolved autonomy at state level. The administrative units are as follows: Federal Capital Territory – Abuja; State – autonomous government; LGA – equivalent of a district: Ward level – equivalent of a sub-district; and Village. The Nigerian Nutrition Sector is led by the Federal Ministry of Health (FMoH) through the Department of Family Health under the Division of Nutrition. Sector coordination has always been and remains led at Abuja level for the three states of the north-east (Adamawa, Borno and Yobe State). Currently, national/federal coordination is chaired by the Director of Nutrition and meetings are held every month. Coordination at state level takes place through meetings chaired by the Director of the Primary Health Care Development Agency (PHCDA) in each of the three states – monthly in Yobe and Adamawa and every two weeks in Borno. The additional sector coordination support provided capacity for the existing coordination forum to engage in context analysis, partner response planning, technical development and information management.
A need to reinforce the coordination of the response in the north-east while ensuring linkages with the federal coordination arrangement was identified. Sector partnerships were growing, with most partners having presence in the north-east but with no representation in Abuja; hence they were absent from national-level coordination. This led UNICEF as cluster lead agency to request surge support from the Global Nutrition Cluster standby partner to add a sector coordination support position in Maiduguri in August 2016 for three months. After the three-month deployment it became clear that the centre of coordination had shifted from Abuja to the State; this led the position to support coordination primarily in the north-east, with monthly support to national coordination. The sector coordinator spends most of their time in Maiduguri, the capital of Borno State (with some travel to Yobe and Adamawa), and one week a month in Abuja to support national coordination meetings and other FMoH-led initiatives.
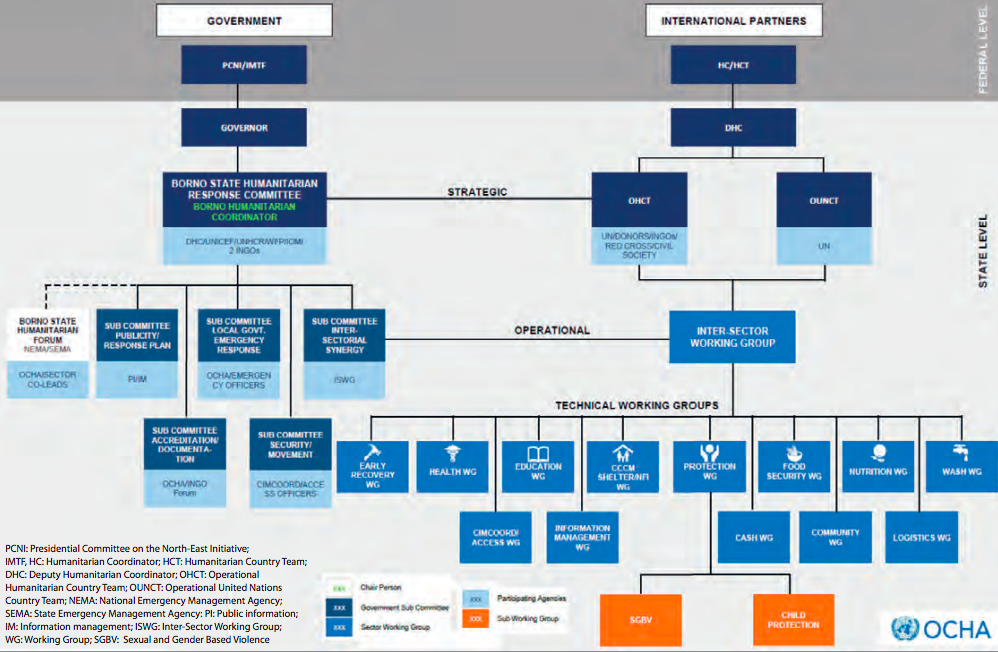
The coordination architecture in NE Nigeria (described in figure 3) is unique in terms of the classic cluster approach, which is often put in place specifically for the emergency response. The cluster approach usually involves a parallel mechanism, led by one specific member of staff hosted by UNICEF and co-led by government and/or a non-government organisation (NGO). The decision was made not to activate the cluster system but instead build on on-going development coordination mechanisms and guide them on humanitarian response coordination. The Nutrition in Emergencies Working Group (NiEWG) was established through dialogue with the Government, who recommended the use of sector rather than cluster. As a result, sector coordination of the emergency response was strengthened with UNICEF as co-cluster lead, with support from partners.
The devolved nature of the health system in Nigeria, given the strong leadership in health by the State Primary Health Care Management Board in Borno State, offered a key opportunity to explore new ways of working to maintain government leadership in coordinating the emergency response. Nutrition was also a key priority under the primary healthcare umbrella. As a result, the approach implemented became a sector coordination-strengthening approach. Initially health and nutrition coordination were merged and chaired by the permanent secretary in Borno Ministry of Health (MoH). As the response requirements grew, the need to establish nutrition-specific coordination was endorsed by the MoH and the State Primary Health Care Development Agency (SPHCDA), the body responsible for provision of primary healthcare, which was mandated to lead the coordination of nutrition activities with support from UNICEF.
The Director of Primary Health Care for Borno SPHCDA, who overseas primary healthcare services (which encompass nutrition services), has been committed to ensuring and directing service delivery in the geographic and technical areas she oversees in order to maintain coherence and strengthen the existing operational and human resource structure of the SPHCDA. In addition, the existing government structure has a dedicated nutrition team led by the State Nutrition Officer with support of four people, including one person dedicated to information and supply management.
State-level meetings are held every two weeks in Maiduguri. As the number of partners increased, with many per each LGA, coordination forums at LGA level were created to improve engagements. These are currently active in five LGAs (Monguno, MMC and Jere, Askira Uba, Dikwa and Banki) and have the specific objective of ensuring that activities are well coordinated, with the ultimate aim of maximising coverage where security permits. These LGA-level coordination units are put in place where there are more than two partners, local or international, and engage the nutrition focal persons from the LGA, with support from one identified partner. The Nutrition Sector-specific LGA coordination mechanisms also link with the United Nations Office for the Coordination of Humanitarian Affairs multi-sector humanitarian coordination hub by attending meetings, which are decentralised at hub level. The state coordination also works with three thematic working groups (TWG) on assessments, community based management of acute malnutrition (CMAM), infant and young child feeding in emergencies (IYCF-E), as well as with task forces to accomplish specific deliverables that have been formed as part of the technical and operation coordination architecture. The TWGs are forums for technical discussions related to the improvement of the response and are led by different partners. These state-level TWGs are linked to the federal-level TWG on some of the issues that need to be managed at federal level.
Figure 3: Nutrition Sector emergency coordination organogram
Achievements of the Borno State Nutrition NiEWG
The role of government in delivering the emergency response and its leadership in facilitating meetings has resulted in several collaborative initiatives for services to be delivered in an increasingly harmonised way. These include:
Geographic mapping at ward level: Ward-level partner mapping of nutrition-related activities has allowed for a better understanding of gaps and identification of duplication, and extension of services in the scale-up process, with corrective actions as indicated (see Box 2).
Nutrition in Emergency Sector Response plan 2017-2018: The response plan is a strategic document on the approach, principles, overall strategies and activities to be implemented, as well as a specific plan with timeframe and deliverables. The response plan links the emergency activities with existing policy and national action plan on nutrition.
Integrated nutrition services – minimum package and modalities of operation: The package was developed by the CMAM TWG and outlines the minimum services in terms of assessments, treatment, prevention and coordination, including an agreed set of indicators for monitoring performance of CMAM programmes. It serves as a guideline and reference to all nutrition programme personnel and partners supporting nutrition services in Borno State. Interventions are mapped and described by service delivery platform, including health facility, community IDP camps, outreach and campaigns. The minimum package was a collaborative effort developed by partners and government, then consolidated by the sector coordinator.
Community nutrition monitor approach: A task force for community mobilisation was formed to review existing approaches and propose a harmonised way forward. A community nutrition monitor approach was developed and agreed by a sub-committee to overcome challenges of coverage and reach of services. The task force agrees on incentives and a minimum set of activities to be performed by monitors, as well as the desired profile for the role.
Scale-up stabilisation care strategy: In view of very low coverage of inpatient services, the CMAM TWG developed a strategy for training hospital personnel and supporting set-up of in-patient nutrition care for cases with medical complications.
IYCF-E statement and strategy: The IYCF-E statement aimed at bringing the need to scale-up IYCF activities and control the use of breastmilk substitutes in the humanitarian response to the attention of the wider humanitarian community. Key successes have been achieved, such as the commitment to withdraw the use of powdered milk as an incentive for children during polio vaccinations. Finalisation of a reporting template and rollout of training of health workers has increased the reporting rate of IYCF activities. The statement and strategy are at final stages of endorsement.
Harmonised approach to human resources (HR): With many partners in Borno employing various incentive schemes and occasionally hiring paid health workers already employed by government, there was a clear need to harmonise the HR approach. The Director of PHC requested that all partners submit their staff incentive system approach and a list of employees to cross-check that they were not already receiving a salary. Partners were also required to request a letter of discharge from health employees applying for positions if they were selected. The objectives were to prevent double pay and the diverting of government workers from their station duties. The link between nutrition and health is made through the Director of PHC, who oversees both nutrition and health as part of routine services. The HR taskforce also managed to harmonise the monetary incentives given to the community nutrition volunteers. Challenges remain in having all partners function through one standardised system/approach and efforts are ongoing.
Sector information database: This includes mapping of partners and interventions at ward level; CMAM and IYCF databases for compilation of sector results; and harmonised reporting systems.
Joint monitoring approach: Government and partners form joint teams for monitoring visits and use a monitoring form that has been validated by sector partners for visits. Several joint monitoring visits have been conducted, with corrective action taken to strengthen the response. The outcome of the joint monitoring has been appreciated as the tools are harmonised and the corrective action agreed by all stakeholders.
Task force for monitoring misuse of nutrition commodities: The task force was established to support sector partners in enhancing monitoring and reporting misuse of ready-to-use therapeutic food (RUTF). Reporting templates were developed and sensitisation carried out with local leaders and health workers. Stock management was also strengthened, with supplies delivered directly bi-weekly to the health facilities based on numbers of children in the programme.
Establishment of the nutrition surveillance system and increasing nutrition assessments: Nutrition assessments were conducted annually and figures for prevalence at state level calculated; the lack of disaggregated data limited informed programme decision making and response planning. Through discussion with the Food and Agriculture Organization, the Center for Disease Control, World Food Programme and UNICEF, the sector developed the nutrition and food security surveillance system (NFSS). Initiated in October 2016 and covering the three north-eastern states affected by the conflict, assessments are conducted three times a year. To date, three rounds of data collection have been completed and have informed the humanitarian needs overview.
CMAM guideline review workshop: The CMAM TWG in Borno convened a workshop to identify key gaps in current CMAM guidelines and to incorporate the management of moderate acute malnutrition. The TWG has the support of the state and the federal government, with assurances of ministerial commitment to review the guideline and incorporate the missing elements.
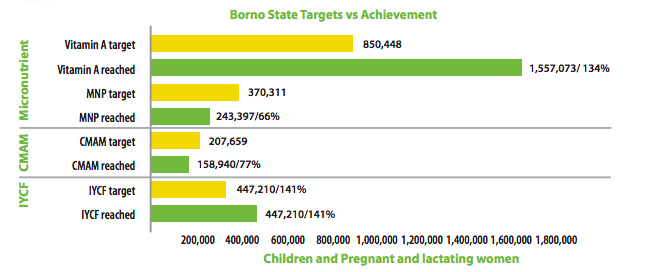
The sector coordination group (Nutrition in Emergencies working group) is dynamic and will continue to address the need for guidance as these emerge and are agreed as a priority by partners. The government leadership has resulted in tripartite partnerships between government, international NGOs (INGOs) and UNICEF to ensure quality of services delivered. In this partnership, the state government provides the health infrastructure and the health workforce; UNICEF provides technical support to the state, fundraises and manages the supply of RUTF and therapeutic commodities for the sector; and INGOs focus on supporting the state with operational capacity and technical mentoring. Figures 4 and 5 illustrate the achievements of the response in numbers in Borno State.
Box 1: Achieving successful partner coordination in Monguno
In October 2016, a geographic mapping was undertaken of nutritional services being delivered by MoH staff with support of partners in Monguno. Interventions had started in July 2016 with primary healthcare and nutritional centres being established with support from UNICEF; there were no existing health services, since the population was displaced into camps, thus services were set up with MoH. Following additional assessments, MSF-France, ALIMA, Action against Hunger and the International Rescue Committee also established CMAM and IYCF services. As a result it was found that some supported facilities were closely located and covered the same population. The Director of PHC, with support of the sector coordination, requested that the situation be resolved to stop the duplication of services. The sector coordinator had a number of meetings with partners to see how to best merge or handover facilities in close proximity. As a result all partners agreed on a strategy. In view of the arrival of partners in the area, UNICEF handed over all its supported facilities, while partners merged or exchanged locations for geographic coherence. The task was challenging yet successful and there is now a forum through which partners exchange and coordinate activities.
Figure 4: Nutrition Sector achievement in numbers, Borno State

Figure 5: Nutrition Sector achievements by intervention in numbers, Borno State
 Challenges and lessons learned
Challenges and lessons learned
Despite many successes of the coordination approach, there have been challenges and lessons learned.
Competition for space between partners led to limited sharing of information and sometimes launching of activities without informing the coordination forum. Proposals were developed for specific locations already covered by a partner. This led to temporary duplication of activities until it was resolved with support of the state. The key lesson here is twofold: first, the need for partners to ‘play the game’ and inform government and sector coordination of their planning; secondly, the importance of donors coordinating their support, being flexible and requiring that projects that are being funded are coordinated through the sector. All activities fall under the Humanitarian Response Plan and are externally funded. There is some consultation by donors with the coordination forum which can be further refined.
Competing priorities within government are important to consider as the Director of PHC also oversees several other primary healthcare-related units. While this oversight is conducive to integration, programmes are delivered vertically, which poses a challenge to integration. The state nutrition team and UNICEF-supported structure have both been vital components in maintaining regular activity of the group.
Low partner commitment on coordination activities has been a constraint. With new partners arriving to set up a response, humanitarian coordination was not always prioritised and was a new phenomenon for some, which limited their participation in coordination activities and contributions to TWGs.
Several factors enabled the government-led coordination mechanism to take shape in Borno State, including strong high-level leadership, political will for an effective response and HR structures to support the work involved in coordination. The focus of the coordination has been mainly on emergency partners, despite the availability of a wider range of development funding throughout other areas of the country. When enabling factors are in place, it is best to empower government and co-lead in strengthening sector coordination in the emergency response, rather than engage in parallel structures.
Conclusion
The experience of the Nutrition Sector coordination in emergencies in Borno State demonstrates that it is possible to work effectively through existing systems. In view of the linkages between development and humanitarian interventions, there is increased need to adapt approaches to specific contexts and local systems. Such experiences demonstrate further prospects for sustainability during and after a humanitarian response.
For more information, contact: Maureen Gallagher or Kirathi Reuel
References
IOM, 2017. International Office for Migration (IOM) Data Tracking Matrix Round XVIII (2017).
National Bureau of Statistics (NBS)/ UNICEF (2010)
National Bureau of Statistics (NBS)/ UNICEF (2012)
World Bank Group. 2015. North-East Nigeria Recovery and Peace Building Assessment: Synthesis Report. World Bank, Abuja, Nigeria. © World Bank. https://openknowledge.worldbank.org/handle/10986/25791 License: CC BY 3.0 IGO.