
Piloting the C-MAMI approach in the Rohingya response in Bangladesh
By Anne Marie Kueter, Alice Burrell, Sarah Butler, Mostofa Sarwar and Habibur Rahaman
Anne Marie is a nutritionist with over five years’ experience in humanitarian nutrition in various countries in Africa, Asia and the Middle East with GOAL, Action Against Hunger and Save the Children UK. She currently works part time as a consultant for Save the Children US and part time as a nutrition adviser for MSF Brussels.
Alice Burrell is a Nutrition Adviser with Save the Children’s Humanitarian Surge Team. She has substantial experience leading on infant and young child feeding in emergencies interventions in the European migrant response, South Sudan, Bangladesh and Syria.
Sarah Butler is the Director of Emergency Nutrition at Save the Children, USA. She has more than ten years’ experience in nutrition across multiple contexts, supporting quality programming and innovation for children.
Mostofa Sarwar is a medical doctor with five years’ experience in maternal and child health and nutrition in development and emergency contexts with leading non-governmental organisations. He is currently the Deputy Manager, Health, Nutrition and HIV/AIDS for Save the Children in Bangladesh.
Habibur Rahaman has a public health background, with over eight years’ experience in emergency and development contexts in Bangladesh. He has previously worked with Action Against Hunger and UNICEF and is currently the Technical Manager Nutrition for Save the Children for the Rohingya response in Cox’s Bazar.
The C-MAMI programme in Cox’s Bazar, Bangladesh, was made possible with the generous funding of DFID (through UNOPS) and UNICEF.
Location: Bangladesh
What we know: Community-based management of uncomplicated severe acute malnutrition in infants under six months is recommended by WHO; the community-based management of at risk mothers and infants less than 6 months (C-MAMI) Tool was developed to help put this into practice.
What this article adds: A pilot programme was implemented by Save the Children and UNICEF in the Rohingya response to identify and manage nutritionally vulnerable infants <6m using an adapted C-MAMI Tool. Seven C-MAMI sites were established between November 2017 and July 2018, integrated/aligned with existing programmes. Infants <6 months and their caregivers were referred via multi-sector community mobilisers for screening and management or referral. By mid-June 2018, 1,964 infant-mother pairs were referred to C-MAMI sites, of whom 762 were enrolled in outpatient care and 78 complicated cases referred for inpatient treatment. Programme challenges included lack of baseline caseload data (anthropometry of infants <6m not included in surveys conducted); the recruitment of suitably qualified staff (MAMI counsellors); high caseload numbers; assessment difficulties (including of low birth weight infants and maternal mental health problems); harsh conditions; data collection difficulties linked to Commcare platform; and some limitations in adaptation of the C-MAMI Tool for this context (discharge criteria). Developments planned include management of simpler cases by existing infant and young child feeding (IYCF) programme to reduce MAMI caseload and transfer to KOBO platform for data collection. Experiences have informed the latest C-MAMI Tool (Version 2). Plans are to scale up MAMI across the Rohingya response.
Background
Acute malnutrition in infants under six months old
In 2017, wasting (both moderate and severe) continued to threaten the lives of an estimated 50.5 million (7.5% of) children under five years old globally. Of these, 16 million were severely wasted (UNICEF/WHO/World Bank Group, 2018). It is estimated that malnutrition was an underlying factor in almost half of the 5.6 million under-five child deaths in 2016 (UNICEF, WHO and World Bank, 2017). These global estimates are largely based on country-level data sets comprised of representative household surveys, within which disaggregated data for infants under six months (infants <6m) are not always available or usually presented. Infants <6m have traditionally been considered less vulnerable to malnutrition due to the protective factors of exclusive breastfeeding; however, only two in five infants <6m are exclusively breastfed globally (UNICEF, 2018) and infants in this age group are often exposed to risky feeding practices (such as unsafe artificial feeding, pre-lacteal feeds and early introduction of complementary foods).
There is now evidence that acute malnutrition is a serious public health concern in the <6m age group. A 2011 secondary data analysis in 26 high-burden countries estimated that 23% of overall SAM cases were infants <6m (Kerac et al, 2011), while a recent secondary data analysis found that infants <6m were at greater risk of death during inpatient treatment than older age groups (Grijalva-Eternod, 2017). Commonly used survey methodologies, such as SMART, typically only collect anthropometric data for children 6-59 months old. One of the complications in getting data for the <6m age group is that there is no internationally agreed cut-off threshold for MUAC to identify at-risk infants. Weight-for-length z-score (WLZ) is the current recommended anthropometric criterion for severe acute malnutrition (SAM) in infants <6m. However, weight and length are more difficult to measure accurately in younger infants and WLZ is not available for lengths under 45cm; therefore this age group is often overlooked in community screenings and nutrition surveys (Lopriore et al, 2007).
Community based management of acute malnutrition in infants
Over the last decade, the management of acute malnutrition in children aged 6-59 months has greatly improved following the introduction of Community-based Management of Acute Malnutrition (CMAM). However, management of acute malnutrition in infants <6m has not kept pace. The 2013 World Health Organization (WHO) Updates on the Management of Severe Acute Malnutrition in Infants and Children recommends for the first time that infants <6m with uncomplicated malnutrition are managed as outpatients, while also acknowledging the low level of evidence to identify and manage cases.
Save the Children pioneered research on the management of acute malnutrition in infants <6m at the community level in Bangladesh from 2013-2016. In 2015 Save the Children collaborated closely with ENN and the London School of Hygiene and Tropical Medicine (LSHTM) in the development of an innovative C-MAMI (Community Management of At risk Mothers and Infants) Tool to help harmonise and catalyse case management (Box 1). The need to address infants <6m in the Rohingya response, coupled with Save the Children’s experience with C-MAMI in Barisal District, Bangladesh, led to the piloting of the C-MAMI approach in this emergency from 2017 to 2018, the results of which are described in this article. These experiences were used to inform the development of the recently released version 2.0 of the C-MAMI Tool1 (see article in this issue).
Box 1: C-MAMI Tool in Bangladesh
The C-MAMI Tool was developed to identify vulnerable infants <6m and their mothers at risk of malnutrition. Assessment and classification of vulnerability do not solely rely on anthropometry as seen in older children, but include feeding, clinical and maternal mental health status to reflect associated risks of mother-infant pair and wider scope of interventions needed to cater for/support them.
Save the Children’s C-MAMI project uses a mobile based application called Commcare to collect and transfer data from the C-MAMI sites to a central, cloud-based database. This application is used for case screening, step-by-step case management and reporting for real-time data collection and monitoring.
The mobile-based system for the assessments automatically classifies the infant and mother according to four colour-coded categories, from severe problem (pink) to moderate and some problem (yellow 1 and yellow 2) to not urgent (green). Infants and mothers classified as pink are referred for inpatient care. Yellow cases are enrolled in the C-MAMI programme and green cases are discharged with general advice only.
C-MAMI in the Rohingya response in Bangladesh
Nutrition situation in the Rohingya population in Bangladesh
According to the Inter Sector Coordination Group report from June 2018, 706,364 Rohingya people have crossed into Bangladesh since 25 August 2017, fleeing large-scale violence in Rakhine State, Myanmar. The Rohingya people have sought safety in Cox’s Bazar (where the total Rohingya population is now 914,678) and are concentrated within Ukhia and Teknaf, where most refugees live in makeshift shelters in congested camps and settlements. SMART surveys conducted between October and November 2017 measured the prevalence of acute malnutrition in children aged 6-59 months by WHZ and found a prevalence of SAM of 7.5 % (95% CI 4.9-11.2) in Kutupalong camp; 3.0% (95% CI 2.2-4.2) in the Makeshift camps; and 1.3% (95% CI 0.5-2.9) in Nayapara camp. WHZ was not measured in infants <6m; however MUAC was assessed to help build the evidence base for this indicator in this age group2. Average MUAC for infants <6m was 118 mm in Kutupalong, 119 mm in makeshift camps, and 118mm in Nayapara. IYCF indicators assessed during the SMART surveys were found to be poor, with only 56.1% of infants <6m being exclusively breastfed in makeshift camps. In Nayapara, exclusive breastfeeding rates for infants <6m were found to be slightly better at 72.2%. The results of the SMART surveys showed that the high levels of malnutrition and poor IYCF practices were further compounded by poor care practices and micronutrient deficiencies.
An estimated 8,129 infants <6m were among the Rohingya camp population, according to a UNHCR family count in late 2017. Despite the absence of survey data on infants <6m to estimate the actual caseload, the relatively high number of infants <6m in the population, coupled with poor IYCF practices and the lack of interventions addressing this particular group, led the Nutrition Sector in Cox’s Bazar to identify the management of vulnerable infants <6m as a gap. A pilot of the C-MAMI approach was endorsed to address this. In November 2017 Save the Children, in partnership with UNICEF, began to implement C-MAMI to address the need for outpatient treatment of nutritionally vulnerable infants <6m, starting with a pilot phase to adapt the methodology to this particular emergency context.

Intervention
The key objectives of the C-MAMI pilot were to test the suitability of the existing tools for use in the Rohingya response to get a better understanding of specific breastfeeding challenges in this context and to determine staffing needs to further inform the training package needed. Supervision visits and lessons-learned meetings were held at each of the C-MAMI sites.
During the original pilot phase (November 2017 to February 2018), four C-MAMI sites were established by Save the Children in Cox’s Bazar. The implementation of the C-MAMI project continued beyond the pilot phase and an additional three C-MAMI sites were opened between March and May 2018, bringing the total of active C-MAMI sites to seven (as of July 2018). All C-MAMI sites are integrated within Save the Children’s wider health and nutrition programme; all sites were set up within mother-baby areas (MBAs) and adjacent to outpatient therapeutic programmes (OTPs) (in all but one of the sites) and health posts. This integrated set-up facilitated the identification and referral of infants <6m and their mothers at facility level; for example, referral of infants and their mothers to the C-MAMI sites from postnatal care services.
The C-MAMI project in Cox’s Bazar is managed by an international senior programme manager and two national programme managers, with support from an international technical adviser. Each C-MAMI site is staffed by two MAMI counsellors (all female) and each site has a MAMI supervisor (both male and female). MAMI counsellors are responsible for screening, anthropometry (weight-for-length (to identify acute malnutrition) and MUAC (for data purposes)), enrollment and registration of mother-infant pairs, and management of enrolled cases including one-to-one counselling. MAMI supervisors are responsible for daily supervision, quality monitoring and on-the-job training and support, as well as reporting of data. An initial training of trainers (ToT) was conducted by an experienced Save the Children staff member from the research project in Barisal. Staff trained during this ToT were then responsible for training new staff as new sites opened.
Identification and referral of nutritionally vulnerable infants <6m and their mothers at the community is supported by multi-sector community mobilisers. Due to the high workload of the community mobilisers and difficulty in identifying vulnerable infants <6m (lack of MUAC cut-off threshold to identify acute malnutrition in infants <6m and assessment of mother-infant pairs for nutritional vulnerability being time-consuming), it was decided that community mobilisers should refer all infants under <6m in the catchment areas of the C-MAMI sites for assessment at facility level. Infants <6m and their mothers were also referred from the health and nutrition posts, especially from the reproductive health units and MBAs. Maternal and child health and nutrition (MCHN) promotors supported the MAMI counsellors with home visits, follow-up, and community health and nutrition education.
Identified nutritionally vulnerable/at risk infants <6m and their mothers were enrolled in the C-MAMI programme. Low-risk infants and their mothers were referred to the IYCF services in the MBAs. In areas where blanket supplementary feeding programmes (BSFP) were available, caregivers of infants <6m were referred to enroll for a supplementary food ration. When infants in the C-MAMI programme turned six months of age they were referred to the appropriate nutrition services (CMAM) for further treatment if necessary.
Results
From November 2017 until mid-June 2018, 1,964 infants <6m old across the seven sites in Save the Children’s catchment area were referred for rapid assessment at the C-MAMI sites3. A total of 847 infants <6m underwent the full mother-infant pair assessment, from which 762 mother-infant pairs were enrolled in the C-MAMI programme. See Tables 1, 2 and 3 below for further details.
Table 1: Classification of mother-infant pairs who underwent full assessment
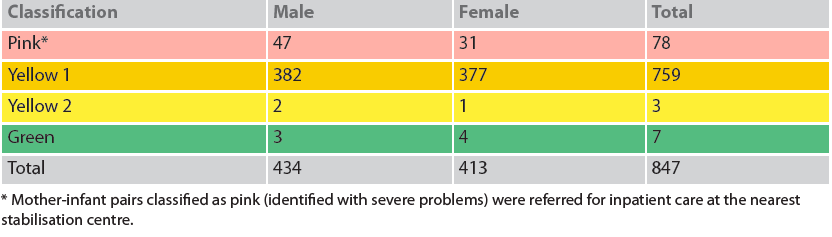
Table 2: Number of infants per age group and average MUAC per age group of infants <6m who underwent full assessment

Table 3: WLZ of infants <6m who underwent full assessment

Until mid-June, 65 mother-infant pairs enrolled recovered, where recovery was based on having all components of the assessment for both infant and mother classified as green (clinical, feeding and anthropometric assessment for both infant and mother, and additional mental health assessment for mother). Recovery was low due to discharge criteria not being fit for the emergency response (see Challenges below). A total of 43 mother-infant pairs defaulted and one infant died.
From 78 infants referred for inpatient care, 14 were identified with SAM and eight with MAM based on WLZ criteria (remaining 58 cases had other clinical complications necessitating inpatient care).
All but one of the 847 infants were breastfed; however common breastfeeding problems such as infants not being well attached and not suckling well and infants receiving less than eight breastfeeds a day were commonly reported and contributed to a large proportion of mother-infant pairs being classified as having a ‘moderate’ problem. According to the assessment of maternal mental health, 3.1% (n=26) of mothers showed signs of depression/anxiety and 3.9% (n=33) indicated having a marital conflict contributing to poor mental health.
Challenges
Field teams identified several challenges during the pilot phase of the C-MAMI approach in the Rohingya response. Firstly, it was challenging to recruit qualified staff – MAMI counsellors in particular – who had to be experienced IYCF counsellors, female and able to speak the local language. Competition with other NGOs for qualified staff further hampered this process and led to a delay in opening of some sites. To help overcome this, during later stages of the project when new C-MAMI sites were opened, Save the Children ‘transferred’ high-performing IYCF counsellors from the IYCF programme to become MAMI counsellors.
High caseload numbers per site were challenging for the MAMI counsellors, especially because of the time needed for close follow-up and weekly monitoring. Enrollment was often found to be due to breastfeeding issues that could be addressed through less intensive IYCF programming in MBAs; i.e. one-to-one breastfeeding counselling providing skilled support with good positioning and attachment. Referral of severe cases was hampered by lack of accessible inpatient services and a general unwillingness of caregivers to stay in the stabilisation centres.
Specific challenges were identified related to the assessment of both mothers and infants. It was difficult to measure/identify low birth weight (LBW) infants due to the lack of health cards and the lack of a growth-monitoring programme, especially at the beginning of the response. MAMI counsellors had limited capacity (knowledge and experience) to identify risk of HIV and tuberculosis and integrated management of childhood illness (IMCI) danger signs. It was also challenging for MAMI counsellors to conduct depression/anxiety assessments and classify this appropriately; some of the standard classifications were felt to be inappropriate for this emergency context. At the time of the pilot, few mental health and psychosocial support (MHPSS) services had been put in place, limiting referral pathways for at-risk mothers. It was sometimes difficult to measure mothers’ MUAC due to a lack of sufficiently private space to remove clothing.
The harsh conditions in the camp (sun, heat, dust during the dry season, and rain and mud during the monsoon season) affected the electronic weighing scales and good-quality anthropometric equipment was not available in the local market.
Despite good community mobilisation, the programme suffered from high numbers of absentees due to the programme not providing any material goods or incentives and it was often difficult for the community mobilisers and MCHN promoters to locate and follow-up all absentees/defaulters (reliable data on defaulters are unavailable due to data errors).
Commcare software was used in the programme to gather MAMI data. However, the free version of the software used did not facilitate easy analysis of data and created discrepancies with the other nutrition programmes, which all used KOBO for data entry and reporting. Additionally, the level of data collected through the Commcare system was excessive for an emergency response, with the extensive variables collected on a weekly basis for each mother and infant more suited to a stable/research setting.
In adapting the C-MAMI Tool for the response, several limitations of the tool itself were identified. The C-MAMI Tool did not accommodate the registration of orphaned infants; the only option provided is to register the infant as ‘with mother’. Re-enrollment is not recorded in the C-MAMI Tool. The discharge criteria were unclear and difficult to implement in the context of this emergency. For example, the C-MAMI Tool specified that the mother’s nutritional status needs to be improved before the mother-infant pair can be discharged; however, food and nutrition security was a problem in the Rohingya response, which was beyond the scope of the C-MAMI programme (aside from education and messaging). This meant that infants and their mothers were kept in the programme for a long period of time. The requirement for an infant to be feeding at least eight times per day pre-discharge also extended stay. This meant it was challenging for the MAMI counsellors to decide when to discharge and contributed to long lengths of stay, which increased risk of defaulting.
More broadly, a key challenge with the C-MAMI intervention is lack of baseline caseload data for this age group. WHZ was not assessed in this age group in the SMART surveys (it is highly challenging for community-level assessment in this age group), and while MUAC is practical and was measured, there are no recommended MUAC thresholds for infants<6m. No additional anthropometric data have been collected on this age group in the latest SMART survey. An in-depth IYCF-E assessment is being planned for September/October 2018, looking at both qualitative and quantitative indicators; there may be potential to gather data that can inform the C-MAMI plans and programmes.
Lessons learned
Despite the gaps in quantitative caseload information, the number of SAM cases identified (9.2% of infants <6m who underwent a full assessment) and the number of mother-infant pairs at high risk who were referred for inpatient management clearly showed the need for an intervention at community level for this vulnerable age group.
The pilot revealed the need to adapt the C-MAMI programme to work alongside an IYCF programme with prioritisation of cases needing specialised support for enrollment in the C-MAMI programme, and other simpler cases managed under the IYCF programme.
Due to several issues with the CommCare platform during the pilot phase, the programme is transferring to KOBO Collect, a more user-friendly platform for which there existed in-house expertise and which is already used in Save the Children’s nutrition programme.
The pilot in the Rohingya response in Bangladesh has directly informed adaptations to the C-MAMI Tool, now reflected in version 2.0, to address gaps (such as discharge criteria), and to help to adapt and apply the tool in an emergency setting. Version 2.0 will be used to simplify the database to gather only crucial data found useful during the pilot phase and for future emergency response settings.
Ways forward
The goal of the pilot phase was to develop a context-specific approach for the identification, management and follow-up of nutritionally vulnerable infants <6m in the Rohingya response. Given the burden identified through the pilot programme, Save the Children in collaboration with UNICEF are planning a response-wide roll-out of the C-MAMI approach across the Rohingya refugee camps, including identification of other health and nutrition actors capable of implementing C-MAMI. To facilitate this, a Save the Children C-MAMI consultant will design a comprehensive roll-out strategy in line with Cox’s Bazar Nutrition Sector priorities, including plans for response-wide monitoring and evaluation, and develop and conduct a ToT for partner staff adapted to the C-MAMI Tool Version 2 and to the emergency context, based on the lessons learned from the pilot phase. The consultant will also document lessons learnt from Save the Children’s ongoing C-MAMI programme and provide suggestions to improve quality.
An outstanding critical impediment to programming planning, monitoring and scale-up is lack of community-friendly indicators to identify at-risk infants in the community, both in surveillance and for assessment by community-level workers.
For more information, email Anne Marie Kueter.
References
UNICEF/WHO/World Bank Group Joint Child Nutrition Estimates (2018) Levels and trends in child malnutrition. Available from: www.who.int/nutgrowthdb/estimates2017/en/
UNICEF, WHO and World Bank UN Inter-Agency Group for Child Mortality Estimation 2017. Levels and Trends in Child Mortality Report 2017. Available from: www.unicef.org/publications/index_101071.html
Lopriore C, Dop MC, Solal-Celigny A and Lagnado G. (2007) Excluding infants under 6 months of age from surveys: impact on prevalence of pre-school undernutrition; Public Health Nutr. 2007 Jan;10(1):79-87.
Kerac M, Blencowe H, Grijalva-Eternod C, McGrath M, Shoham J, Cole, TJ and Seal A. (2011) Prevalence of wasting among under 6-month-old infants in developing countries and implications of new case definitions using WHO growth standards: a secondary data analysis. Arch Dis Child 2011;96:1008-1013.
Grijalva-Eternod CS, Kerac M, McGrath M, Wilkinson C, Hirsch JC, Delchevalerie P, Seal AJ. Admission profile and discharge outcomes for infants aged less than 6 months admitted to inpatient therapeutic care in 10 countries. A secondary data analysis. Matern Child Nutr. 2017 Jul 25. doi: 10.1111/mcn.12345.
UNICEF (2018) Adopting optimal feeding practices is fundamental to a child’s survival, growth and development, but too few children benefit. Available from: https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/
Endnotes
1Available at www.ennonline.net/c-mami
2As encouraged in the January 2018 meeting of the MAMI Special Interest Group. See www.ennonline.net//resources/mamisigmeetingreport2018
3Screening/referral from community mobiliser in the catchment area was considered to have good coverage but was not formally measured due to challenges. Exact catchment populations in the areas of operation are unknown. While information per zone is available, Save the Children facilities do not always cover the whole zone and are sometimes on the border between different zones, making it hard to generate accurate figures.